Chapter 3: Health and Wellbeing
About this document
Lead authors: Dann Mitchell, John Newton
Contributing authors: Neil Adger, Dan Bernie, Kerry Brown, Catherine Butler, Charlie Dearman, Julia Fussell, Emma Gillingham, Joanne Godwin, Matt Lloyd Jones, Frank Kelly, Sari Kovats, Owen Landeg, Eunice Lo, Andy Morse, Ellie Murtagh, Helen Onyeaka, Cat Pinho-Gomes, Tim Taylor, Grace Turner, Monika Walia, Ben Wheeler
Additional contributors: Selina Dagless, Gemma Holmes, Owen Bellamy, Daniel Williams
This publication is available in PDF format at the end of the page >
3.1 Chapter summary
Health and wellbeing encompasses all aspects of acute and chronic human health that are sensitive to changing weather and climate patterns, including their extremes. Outcomes span both physical and mental health, and include fatalities, injuries, hospitalisations, and exposures. The chapter assesses both the direct risk from weather, including heat, flooding, drought, storms, wildfires, and the indirect risk, via air pollution, infectious diseases, and food safety and nutrition. The purpose of this chapter is to consider the overall health burden of climate change to the UK, and how adaptation can reduce that burden.
Headlines
- Risks to health and wellbeing identified in the previous Climate Change Risk Assessment Technical Report, CCRA3-IA TR, persist and the need for action to address them is now more urgent, based on new evidence.
- For health and wellbeing, the highest urgency risk is from heat (H1), where critical action is needed.
- Substantial risks to the health and wellbeing of people also come from poor air quality (H3), which requires critical investigation, and from flooding (H2), new and existing climate-sensitive infectious diseases (H4) and from disruptions to health and social care delivery (H6), where more action is needed.
- Across all risks to health and wellbeing, heat acts as a compounding hazard.
- Young children, elderly people, pregnant people, people on low incomes, and people with underlying health conditions were consistently the most vulnerable groups to all risks assessed as needing critical action or critical investigation.
- Insufficient evidence is available for deep assessment of cause-specific mortality (mortality broken down by specific diseases or injuries), non-lethal health outcomes, or chronic health outcomes from delayed or long-exposures (years to decades) to hazards.
- Assessment of health benefits from adaptation measures is limited because many are not yet in place, are too new to evaluate properly, or lack suitable assessment methodologies. The strongest evidence of benefit comes from building design, greening co-benefits, and adverse weather messaging.
Risks to health and wellbeing identified in the Third Climate Change Risk Assessment – Independent Assessment Technical Report (CCRA3-IA TR) persist and the need for action to address them is now more urgent. This is because of new evidence linking poor health and wellbeing to climate change, and because the increased warming in the last five years has led to stronger evidence linking climate change and health issues. Changes in substantial action to mitigate the risks have been limited or absent. While the evidence base has evolved, there are still many gaps in our understanding.
Risks arising from heat (H1) have been assessed as Critical action needed for the UK. Increases in heat and heat extremes pose a significant health threat, with specific evidence for England, Scotland, and Wales. This threat is apparent in outdoor and indoor settings and can threaten health and social care delivery.
Risks to health from the climate change component of poor air quality (H3) needs critical investigation. While the total health burden from poor air quality is substantial, the component driven by physical climate change (e.g., high temperature) is highly uncertain owing to the deep interconnections between air pollutants and climate.
It was determined there is more action needed across the UK for risks from other types of extreme weather (H2), climate-sensitive infectious diseases (H4), and health and social care delivery (H6). The UK is also facing an increased risk of flooding, which poses significant health risks to physical and mental health. Detection of new health-relevant pathogens and vectors in the last five years, especially in England, points toward a growing risk of future outbreaks of diseases, including West Nile virus, dengue, chikungunya, and tick-borne encephalitis. Given a strong association between certain food-borne and water-borne diseases with temperature, the risk of outbreaks for these types of diseases is expected to increase as temperatures in the UK rise.
The evidence base gathered was considered comprehensive for the health risks related to heat (H1), other extreme events (H2), and health and social care delivery (H6). The highest quality of evidence focused on population exposures, or overall deaths related to these risks. However, this evidence generally did not specify the cause of death, such as respiratory or heart failure. Evidence was considerably weaker for non-lethal health impacts, or delayed health impacts associated with long climate exposures.
There is more evidence to determine the magnitude and trend for risks in the current climate than for future scenarios, especially when considering adaptation. There is an urgent need for studies projecting health hazards under future climate scenarios, especially for climate-sensitive infectious diseases (H4), and to a lesser extent for food safety and nutrition (H5). Scenarios that include different potential adaptation pathways are extremely difficult to construct, and as such are largely absent across risks.
Across all risks to health, heat (H1) acts as a compounding hazard. Indoor and outdoor adaptation strategies that address this risk will, in general, reduce the other health threats explored across this chapter. Heat changes land processes, increasing flooding and drought exposure (H2), altering air quality contaminants and exposure (H3), helping infectious diseases spread and grow (H4), including through food safety (H5), and disrupting health and social care delivery (H6).
Critical action for adaptation was identified in the most vulnerable groups across all risks. These include young children, elderly people, pregnant people, people with outdoor livelihoods, people on low incomes and those with underlying health conditions. Adaptation measures that target these groups are needed, including associated infrastructure such as childcare facilities, schools, hospitals, and social care.
Adaptation interventions which promote use of green and blue spaces create opportunities for better physical and mental health. Green infrastructure, such as urban trees, woodlands, and parks, can serve as natural buffers against climate change and extreme weather, reducing higher temperatures felt in built-up areas (known as urban heat island effects), reducing the risks of surface flooding, and filtering out harmful air pollutants. Climate adaptation strategies that enhance the quality, equity, and access of green infrastructure can act as a dual solution for climate resilience and public health.
Table 3.1: List of risks and urgency scores for Health and Wellbeing by country. Details of how the scores in this table were calculated are in the Methods Chapter. | |||||||
| ID | Risk | Present | 2030 | 2050 | 2080 | Urgency | |
| H1 | Risks to people from heat | UK | VH • • • | VH • • • | VH • • • | VH • • • | CAN |
| England | VH • • • | VH • • • | VH • • • | VH • • • | CAN | ||
| Northern Ireland | M • | M • | H • | H • | CI | ||
| Scotland | VH • | VH • • | VH • • | VH • • | CAN | ||
| Wales | H • • | VH • • | VH • • | VH • | CAN | ||
| H2 | Risks to people from extreme weather, excluding heat | UK | H • • • | H • • • | H • • • | H • • • | MAN |
| England | H • • • | H • • • | H • • • | H • • • | MAN | ||
| Northern Ireland | H • • • | H • • • | H • • • | H • • • | MAN | ||
| Scotland | H • • • | H • • • | H • • • | H • • • | MAN | ||
| Wales | H • • • | H • • • | H • • • | H • • • | MAN | ||
| H3 | Risks to people from changes in air quality | UK | VH • | VH • | VH • | VH • | CI |
| England | VH • | VH • | VH • | VH • | CI | ||
| Northern Ireland | VH • | VH • | VH • | VH • | CI | ||
| Scotland | VH • | VH • | VH • | VH • | CI | ||
| Wales | VH • | VH • | VH • | VH • | CI | ||
| H4 | Risks to people from climate-sensitive infectious diseases | UK | M • • • | M • | M • | M • | MAN |
| England | M • • • | M • | M • | M • | MAN | ||
| Northern Ireland | M • • | M • | M • | M • | MAN | ||
| Scotland | M • • | M • | M • | M • | MAN | ||
| Wales | M • • | M • | M • | M • | MAN | ||
| H5 | Risks to food safety and nutrition | UK | M • | M • | M • | M • | FI |
| England | M • | M • | M • | M • | FI | ||
| Northern Ireland | M • | M • | M • | M • | FI | ||
| Scotland | M • | M • | M • | M • | FI | ||
| Wales | M • | M • | M • | M • | FI | ||
| H6 | Risks to health and social care delivery | UK | H • • | M • • | H • • • | H • • | MAN |
| England | H • • | M • • | H • • • | H • • | MAN | ||
| Northern Ireland | M • • | M • • | M • • | H • • | MAN | ||
| Scotland | H • • | M • • | M • • | H • • | MAN | ||
| Wales | M • • | M • • | M • • | H • • | MAN | ||
3.2 Risks to health and wellbeing
3.2.1 Risks to people from heat – H1
This risk considers the current and future risk from extreme heat to the health and wellbeing of individuals. The risk from extreme heat to health and social care delivery (H6), and to buildings and communities (BE1), are considered separately. Nonetheless, their interdependency means that some adaptation solutions would benefit all of them. Risks from other extreme weather (flooding, drought, wildfire and cold) are covered in H2.
Headlines
- Heat is a significant threat that is likely to be exacerbated under climate change. Currently, UK annual heat-related deaths range from 1,400 to 3,000. They are projected to rise to 1,500-4,000 in the 2030s, 3,000-10,000 in the 2050s, and around 9,000 in the 2080s. Population change could double or triple these estimates at the end of the century.
- Evidence for all-cause mortality risk is strong, and evidence for some disease-specific causes is strengthening, such as cardiovascular, renal, respiratory, dementia, and acute mental health conditions. More evidence is needed on long-term exposures for chronic illness, which is potentially significant. Linking primary care and health cohort data to weather and climate exposure data is needed to assess the evidence base for other diseases.
- Over-65s, young children, urban residents, the socioeconomically deprived, pregnant people, those with underlying health conditions, and outdoor workers are the most vulnerable groups in the population.
- Adverse Weather and Health Plans are in place in England and Scotland and are likely to be advantageous for Wales and Northern Ireland, as they are projected to face high to very high risk from the 2050s onward. Urban design, such as building ventilation, and urban forests, are strong adaptation strategies for improving heat-related health.
- The magnitude and urgency score of this risk has mostly increased since CCRA3-IA-TR as there is stronger evidence on disease-specific health outcomes.
| Table 3.2: Urgency scores for H1 Risks to people from heat. Details of how the scores in this table were calculated are in the Methods Chapter. | |||||||
| ID | Risk | Present | 2030 | 2050 | 2080 | Urgency | |
| H1 | Risks to people from heat | UK | VH • • • | VH • • • | VH • • • | VH • • • | CAN |
| England | VH • • • | VH • • • | VH • • • | VH • • • | CAN | ||
| Northern Ireland | M • | M • | H • | H • | CI | ||
| Scotland | VH • | VH • • | VH • • | VH • • | CAN | ||
| Wales | H • • | VH • • | VH • • | VH • | CAN | ||
3.2.1.1 Evidence relevant to the entire United Kingdom
Current and future drivers of risk
High temperatures can contribute to diseases (e.g., cardiovascular, respiratory, renal, skin) (Parker, Mo and Goodman, 2022; Mitchell et al., 2024) and can lead to thousands of deaths in the UK every year. They can also influence the efficacy of medications (e.g., antidepressants), impact wellbeing via altering socialising and sleep patterns (Godwin et al., 2025) and increase domestic and societal violence rates (Hanlon et al., 2021). Heat increases suicide risk (twice the risk at 32 °C versus 22 °C) and can exacerbate the symptoms and medication side effects of psychiatric illness, an illness that affects 16% of the UK population (Environmental Audit Committee, 2023). Heat risks to people’s health and wellbeing are increasing due to climate change (as heatwaves become more frequent and intense; see State of the Climate chapter), increasing exposure (e.g., more people in cities or “urban heat islands” that are hotter than rural areas), and increasing population vulnerability (e.g., due to ageing and increasing prevalence of long term conditions). Hot “summer days” and “tropical nights” (where overnight temperature remains above 20 °C) pose risks to human health and wellbeing, and they are increasing. Tropical nights are rare in the current climate, but southern England and Wales are projected to have an annual average of up to five a year at 4 °C of global warming (Hanlon et al., 2021) and this could be even higher during an extreme hot year (see Fig.1.3 in State of the Climate chapter).
Vulnerability: The very young, older people, people suffering from mental health disorders, and pregnant people are more vulnerable to heat due to having lower physiological capacity (e.g., sweating), lower perception of heat risk, and the need to control their body temperature (Thompson et al., 2024; Nisa and Mahase, 2025). Heat also increases the risk of adverse pregnancy outcomes (Lakhoo et al., 2025). People who have disabilities or underlying health conditions (e.g., cardiovascular, lung, heart, and kidney diseases, diabetes, multiple sclerosis, autonomic nervous system issues, and spinal cord injuries) are also vulnerable (NPC 2023). Those older than 75 are more likely to have pre-existing health conditions, making them vulnerable due to both old age and underlying disease. Low-income communities are also vulnerable, as they tend to live in areas with less green space (which helps reduce heat exposure), and they may have less resources to afford fans or air conditioners compared to wealthier communities. Those who undertake hard labour, especially when working outdoors, are also vulnerable (Autonomy Institute, 2023). In addition, there is increasing evidence of socioeconomic and structural inequalities in the impact of heat, which are strongly associated with differences in housing and working conditions. Population groups experiencing deprivation, such as ethnic minorities, may be more exposed to heat due to their housing and working environments (Thompson et al., 2025).
Risk Interactions: Heat exacerbates poor air quality (H3), increases the spread of some infectious diseases (H4), threatens food safety (H5), and can affect healthcare delivery (H6). Prolonged heat when combined with lack of precipitation can also lead to drought, which carries additional health risks, mainly due to the impact on drinking water supplies. People’s physical exercise may be restricted by extreme heat, and those undertaking or spectating sport face a higher risk of heat stress and heat stroke (DCMS, 2025). Extreme heat is also likely to severely affect the workforce, volunteers and coaches at sporting and physical activity events. However, moderate increases in temperature may benefit outdoor activity and increase usage of green and blue spaces.
Assessment of current magnitude of risk
The current magnitude of the risk is Very High for England and Scotland, high for Wales, and Medium for Northern Ireland, justified primarily by independent empirical heat-related mortality estimates. UK annual heat-related mortality was, on average, 1,400 deaths a year in the period 1990-2019 (Figure 3.1) (Jenkins et al., 2022), with around 800 in England and Wales (2000-2019 period) (Gasparrini et al., 2022).

Figure 3.1. Empirical and projected UK heat-related mortality, assuming no population or adaptation change in future. The 1990-2019 value is based on Jenkins et al., 2022, whereas England values in 2022, 2023 and 2024 are from the corresponding UKHSA annual reports. Projections relate to the high warming scenarios in the 2030s, 2050s and 2080s under the CCRA4 climate framing, and are based on (Jenkins et al., 2022; Murage et al., 2024; Masselot et al., 2025). Error bars indicate the 95% confidence intervals.
Assessment of future magnitude of risk
In the 2030s central warming scenario, annual UK heat-related deaths are projected to rise to around 2,400 (Jenkins et al., 2022). Population growth would increase this to 2,500 deaths, but adaptation could limit this increase to 1,500 deaths. In the 2030s high scenario, heat-related deaths are projected to be 1,500-4,000 a year, assuming no population or adaptation change (Figure 3.1). Population growth would amplify this, and adaptation would decrease this (Jenkins et al., 2022).
No heat-mortality estimates are available for the 2050s central scenario, so the urgency score is based on interpolation between other scenarios in the 2030s and 2050s. In the 2050s high scenario, annual heat-related deaths are projected to be 3,800-10,000 a year (Figure 3.1). High population growth would increase this number, but adaptation would reduce this to 2,200 even with population growth (Jenkins et al., 2022).
No estimates are available for the 2080s low and central scenarios, but annual heat-related deaths are expected to be in the high thousands given the other values in the 2050s and 2080s. In the 2080s high scenario, annual heat-related deaths are projected to be around 9,000 assuming no population or adaptation change (Figure 3.1). Demographic change or population growth would increase this to 10,000-18,000, suggesting a doubling or even tripling of mortality (Cole et al., 2023). Adaptation to increasingly hot temperatures, including individual behaviour, environment, and public health systems, could reduce this number to around 3,400 (Jenkins et al., 2022). These projections are significantly influenced by assumptions of population growth and ageing, as well as the extent of global warming and adaptation.
Studies show that among all heat-related causes of mortality, heat related-cardiovascular and respiratory disease will have the largest future increases, followed by renal disease, drowning and mental health problems (small to medium increases) (Mitchell et al., 2024). Renal disease, sleep and cognitive disorders may be particularly susceptible to persistent exposure to heat over years or decades, whilst skin cancer incidence may also increase due to behaviour adaptation to heat with increased exposure to UV radiation. More research is needed to understand the impacts on chronic health from repeated, persistent, or long-exposure (years to decades) to heat (Mitchell, 2025). There is evidence such exposure can lead to progression of neurological disease, for instance epilepsy and stroke (Gulcebi et al., 2025).
Level of preparedness for risk
The National Adaptation Programme (NAP) is an important mechanism to inform and promote the actions needed to increase heat adaptation (Defra, 2024c), but the Third National Adaptation Programme (NAP3) does not define actions at scale to adapt and instead focuses on research needs. While England and Scotland have implemented Adverse Weather and Health Plans (Public Health Scotland, 2024; UKHSA, 2025a (AWHP)), their effectiveness in, for instance, significantly reducing heat mortality, remains to be evaluated. Wales and Northern Ireland do not have equivalent plans. The Office for National Statistics (ONS) is leading a Climate and Health in Official Statistics project (2022-2026) with UKHSA (ONS, 2024), to estimate local-level impacts. This includes, for example, from extreme weather events, heat-related mortality, non-communicable diseases, respiratory illnesses, and mental health.
Policies and plans to address heat risks to people are mostly reactive rather than proactive (Howarth, 2024). The public, and specifically the vulnerable, often do not recognise their risk and there is limited awareness of protective behaviours against heat (British Red Cross, 2021, 2023).
Assessment of the evidence base and evidence gaps
The risk scores are informed by heat-mortality evidence, but not evidence on morbidity. This is mostly due to data scarcity of e.g., GP data. There is limited evidence of the health impacts of chronic heat exposure, and long datasets will be needed to study them. Future projections focused on changes in exposure and vulnerability are missing, (UKHSA, 2024e (HECC chap.2)).
Box 3.1 Opportunities for health and wellbeing in the UK
As the UK adapts to a changing climate, a growing body of evidence suggests some health and wellbeing benefits can emerge from adaptation actions. These arise via reducing risks and taking advantage of opportunities associated with our changing climate. One area for such opportunity is adaptation to support increased use of, and access to, green and blue spaces. Green spaces include parks, gardens and forests, while blue space refers to rivers, lakes, canals and coasts. Adaptation measures can serve to help maximise the health and wellbeing benefits of green and blue spaces as the climate changes. It is important to highlight that whilst these co-benefits and opportunities exist, the overarching impacts of climate change on health are largely adverse (H1-H6).
Current and future drivers of opportunity: Climate change adaptations that increase access to green and blue spaces present both opportunities and risks for health and wellbeing through increased potential for outdoor recreation and active travel. Warmer weather may encourage greater use of natural spaces; however, antagonistic effects, such as increased rainfall and stronger winds, could reduce this trend. Adaptation measures may therefore support increased opportunities for associated health and wellbeing benefits and/or help to mitigate adverse impacts of climate change on outdoor recreation and active travel. Adaptation measures may also interact with existing vulnerabilities, including significant potential to exacerbate health inequalities. For example, accessibility of green and blue spaces tends to be lower for ethnic minority and low-income communities (Boyd et al., 2018; Natural England, 2025). While the (limited) current evidence available for the UK suggests a linear association with warmer days associated with greater physical activity through outdoor recreational visits to natural environments, extreme heat is likely to act as a deterrent to this activity (and similarly for active travel), especially for more vulnerable groups such as older people and those with existing chronic diseases. It is not as clear how many of the other weather patterns could change outdoor physical activities, but there are several feasible links.
Assessment of current opportunity: Increased access to blue and green spaces offers significant co-benefits. Green and blue space access can deliver a range of physical and mental health benefits such as reducing chronic stress and encouraging exercise (White et al., 2020; Browning et al., 2022). Interventions relating to urban greening include increasing the quantity of green infrastructure such as urban trees, parks and gardens as well as creating a network of connected parks and green spaces (Sharifi et al., 2021). Evidence of improved health related to green spaces from other countries found lower rates of cardiovascular disease, stroke, and mood disorders, with exposure to trees being particularly important (Nutsford, Pearson and Kingham, 2013; Astell-Burt and Feng, 2019; Seo et al., 2019). Trees have been indicated as particularly beneficial – studies of experimental exposure of individuals (e.g., in ‘forest bathing’ interventions) demonstrate reductions in blood pressure, heart rate and cortisol and improvements in negative emotions such as anger, confusion, depression, and fatigue (Cheng et al., 2021; Caryl et al., 2025). Increased recreational visits to blue spaces (inland and coastal environments with water) also creates health and wellbeing benefits (White et al., 2020).
Physical activity during leisure visits to green and blue spaces increases with rising temperature, while wind speed has a negative impact, and precipitation shows no clear association (Elliott et al., 2019). While warmer temperatures may initially encourage more physical activity, this may reverse under extreme heat, especially for vulnerable groups such as older adults, those with existing chronic diseases and those with high Body Mass Index (An et al., 2020; Bernard et al., 2021).
Assessment of future opportunity: Given the limited evidence, the magnitude of the opportunity for outdoor recreation and active travel health co-benefits of adaptation actions in 2050s and 2080s is unclear. There is no specific evidence to inform this, but there may be increasing opportunity by 2080s, as overall higher temperatures by this time could lead to greater opportunities via outdoor recreation and active travel. However, the net effect accounting for any adverse impacts of extreme heat is unknown.
Level of preparedness for opportunity: There are likely to be health benefits of adaptation specific to this opportunity, for example in terms of ensuring the quality and public trust in outdoor swimming waters, given that perception of quality impacts on recreational use. There are also well-established barriers to green/blue space access, including physical constraints and broader social determinants (Boyd et al., 2018; Natural England, 2025). Delivering social and physical environmental adaptations that serve to improve accessibility would be likely to capitalise on the opportunities presented.
Assessment of the evidence base and evidence gaps: Urban green and blue spaces offer critical adaptation functions, and there is a large volume of evidence on how increased green/blue space accessibility might deliver health and wellbeing benefits.
Interventions can involve environmental/infrastructure changes and/or social, educational or health service programmes (Hunter et al., 2019). Nature-based social prescribing programmes provide pathways to promote and support green/blue space access and related activities for individuals with a range of health conditions or risk factors, and recent large-scale evaluations indicate effectiveness for mental health specifically (Defra, 2024b). For example, the NHS Forest delivers an array of interventions aimed at increasing green/blue spaces, biodiversity and tree cover on healthcare sites to promote wellbeing (Centre for Sustainable Healthcare, 2026). The tree equity score tool allows for a targeted assessment of where best to plant trees in built environments, to promote positive health and reduce inequalities (Woodland Trust, American Forests, and Centre for Sustainable Healthcare, 2023). However, further evidence on the complex interaction of different weather conditions, including wind and rain, on nature access, outdoor recreation and active travel is required. Given the importance of local environments, cultures and socio-economic characteristics in shaping these relationships, evidence is required that is specific to the UK and the devolved administrations.
3.2.1.2 England
Assessment of current magnitude of risk
Current risk is Very High, up from high in CCRA3-IA TR (which was the highest risk level at that time). There are thousands of heat-related deaths per year (3,000 in 2022; 2,300 in 2023; 1,300 in 2024) (UKHSA, 2024k, 2025c, 2025d), equivalent to two to five heat deaths per 100,000 people a year. The leading causes for heat-mortality in 2024 were the exacerbation of all circulatory diseases, dementia and Alzheimer’s, and influenza and pneumonia (UKHSA, 2025d). Heat-related mortality is generally higher in London and South East England due to a combination of climate, urban heat island effect, large population and socioeconomic factors such as deprivation and inequalities in greenspace access (Gasparrini et al., 2022; Konstantinoudis et al., 2022; Cole et al., 2024; Jackson and Noushad, 2024; Simpson, Brousse and Heaviside, 2024).
On days above 23 °C, there were three additional GP consultations and nine additional prescriptions per 1,000 registered NHS patients in the period 2007-2019 (Fahr et al., 2025). Hospital accident and emergency attendances surged on hot days (Fahr et al., 2025); and hospital admissions for infectious, metabolic, cardiovascular, respiratory and renal diseases, dementia, cancer, and injuries, increased with high temperatures (Gong, Part and Hajat, 2022; Rizmie et al., 2022; Agewall et al., 2023; Hajat et al., 2024). In particular, there were 110 to 120 heat-related dementia hospital admissions in 2009 (Gong, Part and Hajat, 2022). While this is based on England’s evidence, similar trends may apply to the other devolved administrations (ONS, 2022).
Assessment of future magnitude of risk
Future risk remains Very High. In the 2030s high scenario, assuming no population change or adaptation, projected heat-related mortality is 3,100 deaths a year (Murage et al., 2024). This represents a 41% increase from the average annual heat mortality in the period 2022-2024. Regions most at risk include Greater London, the South East, East of England, the West Midlands, Yorkshire, and Greater Manchester (Jenkins et al., 2022; Murage et al., 2024). Considering a high climate change scenario, and assuming an increase in prevalence of dementia but no increases in adaptation, dementia hospital admissions are projected to increase to around 400-500 a year (Gong, Part and Hajat, 2022). Most of these increases come from the 75-84 and 85+ age groups.
In the 2050s high scenario, heat-related mortality is projected to be around 7,500 a year (i.e., 13 deaths per 100,000 people), with the highest mortality rate in the East of England (Murage et al., 2024). In the 2080s high scenario, climate change and urban sprawl combined with the expected population increase mean regions in Southern and Central England will likely experience 13,400 more annual heat-related deaths than the recent past (Jenkins et al., 2022).
Level of preparedness for risk
England’s Adverse Weather and Health Plan (UKHSA, 2025a) includes the Heat-health Alert Service, jointly provided by UKHSA and the Met Office from June to September, to forewarn health and social care professionals of high temperatures that may affect public health. However, awareness of the alerts varies, and the health sector’s response to heatwaves is affected by competing priorities such as infection control, electric fan usage and patient safety (Brooks et al., 2023). Evidence on the effectiveness of the plan is lacking. Adaptation in prisons and schools has been required by the Ministry of Justice (Ministry of Justice, 2024) and the Department for Education (School Building Requirements for resilience to 2 °C and adaptation to 4 °C warming)(Centre for Sustainable Healthcare, 2026), respectively.
Box 3.2 Opportunities for health and wellbeing in England
There are ongoing efforts in England to improve the quality and access of blue and green spaces. The Environment Improvement Plan (Defra, 2025b) for England is underway, with notable progress through the Green Infrastructure Framework (Natural England, 2023) and associated Standards. A key recommendation is that all residents should live within a 15-minute walk of high-quality green or blue space (Defra, 2025b). Urban forests can help reduce heat-health impacts and have been estimated to avoid around 150 heat attributable deaths from 2015–2022 in London (Taylor et al., 2024). In parallel, the National Planning Policy Framework (DLUHC, 2024) was revised in response to the Levelling-up and Regeneration Act 2023 (HM Government, 2023), further aligning spatial planning policy with climate resilience and social equity goals. The framework recognises economic, social (e.g., healthy communities) and environmental (e.g., adapting to climate change) objectives as equally important and outlines how planning and decision-making should be made to favour sustainable development. Together, these initiatives support climate adaptation while enhancing public health, wellbeing, and environmental quality.
Evaluation of urgency score
There is less information on planned adaptation from the 2050s onwards. Due to the Very High projected risk and the fragmented policy responses, critical action is needed. This score is given with High confidence, given the quantitative evidence from past heatwave impacts in England and robust projections on future impacts.
Table 3.3: Urgency scores for H1 Risks to people from heat for England. Details of how the scores in this table were calculated are in the Methods Chapter.
| England | |||||||||
| H1 | Risks to people from heat. | ||||||||
| Present | 2030 | 2050 | 2080 | ||||||
| Central | High | Central | High | Low | Central | High | |||
| No adaptation | VH • • • | VH • • • | VH • • • | VH • • • | VH • • • | VH • • • | VH • • • | VH • • • | |
| With adaptation | VH • • • | VH • • • | VH • • • | VH • • • | VH • • • | VH • • • | VH • • • | ||
| Urgency scores | CAN | CAN | CAN | MAN | |||||
| Overall urgency score | CAN | ||||||||
3.2.1.3 Northern Ireland
Assessment of current magnitude of risk
Current risk is Medium due to evidence showing around seven heat-related deaths in the July 2018 heatwave and, on average, two deaths a year in the 1981-2000 period (Kennedy-Asser et al., 2025). These numbers are equivalent to 0.1 to 0.4 heat deaths per 100,000 people. Another study suggested potentially no heat-related deaths in summers 1991-2018, but with uncertainty (Huang et al., 2020).
Assessment of future magnitude of risk
Future magnitude from the 2050s onward is High. In the 2050s, heat-related mortality is projected to be around 16 deaths a year (0.8 per 100,000 people), considering both climate and population change (Kennedy-Asser et al., 2025). In the 2080s, this is projected to increase to 22 deaths a year (0.8 per 100,000) in a low climate scenario, and 98-108 deaths (about 4 per 100,000 people) in a high climate scenario (Jenkins et al., 2022; Kennedy-Asser et al., 2025).
Level of preparedness for risk
There is no heatwave plan in Northern Ireland. The Building Regulations, under review by the Building Regulations Advisory Committee convened by the Department for Finance, limit internal thermal gains and require adequate ventilation in all buildings (Department of Finance, 2023). The Department of Communities is developing a new Housing Strategy that will set out targets for new homes. Housing retrofitting is being explored by cities including Belfast City Council (Belfast City Council, 2024). These consultations and strategies remain to be concluded and finalised. The urgency scores are unchanged unless these are implemented.
Box 3.3 Opportunities for health and wellbeing in Northern Ireland
Evidence from the Connswater Community Greenway in Belfast suggests there are mental and physical health benefits of urban green/blue space accessibility in the context of urban greenways, including facilitating physical activity (Wang et al., 2023, 2024). The Environmental Improvement Plan for Northern Ireland (DAERA, 2024a) aims for everyone to connect with and enjoy greenspaces. By 2028, the aim is to have a community trail network and green/blue places plan in all district council areas, along with new fit for purpose outdoor recreation legislation.
Evaluation of urgency score
For current and the 2030s, this projection has changed from High in CCRA3-IA TR, to Medium, due to two new studies both projecting fewer than 10 heat-related deaths per year. Before, there was one study that showed around 20 heat-related deaths (Hajat et al., 2014). Confidence is Low reflecting this disagreement and a small number of studies.
Table 3.4: Urgency scores for H1 Risks to people from heat for Northern Ireland. Details of how the scores in this table were calculated are in the Methods Chapter.
| Northern Ireland | |||||||||
| H1 | Risks to people from heat. | ||||||||
| Present | 2030 | 2050 | 2080 | ||||||
| Central | High | Central | High | Low | Central | High | |||
| No adaptation | M • | M • | M • | H • | H • | H • | H • | H • • | |
| With adaptation | M • | M • | H • | H • | H • | H • | H • • | ||
| Urgency scores | FI | FI | CI | FI | |||||
| Overall urgency score | CI | ||||||||
3.2.1.4 Scotland
Assessment of current magnitude of risk
Current risk is Very High. There are tens to hundreds of heat-related deaths a year, with three out of the four years since 2021 having over 140 deaths (e.g., 160 in 2022). These are equivalent to 0.3 to 3 deaths per 100,000 people (Public Health Scotland, 2025b). A 4% to 7% increase in mortality risk is observed during extreme heat (Wan et al., 2022). Worsened air quality (H3) was recorded in Scotland in recent heatwaves (Scotland’s Environment, 2022), which could have exacerbated the health impact of heat.
Assessment of future magnitude of risk
Future risk is Very High. In the 2030s, assuming no population change, heat-related mortality is projected to be around 150 deaths a year (three deaths per 100,000 people (Murage et al., 2024)). In the 2050s, this is projected to increase to 410 deaths a year (8 deaths per 100,000 (Murage et al., 2024)). In the 2080s, Scotland is projected to have around 420 more annual heat deaths than in the past few years (Jenkins et al., 2022).
Level of preparedness for risk
Public Health Scotland has an Adverse Weather and Health Plan for 2024-2027 that covers heat (Public Health Scotland, 2024). It includes developing a real-time surveillance system, scoping potential development of heat-health alerts, developing a collection of guidance for health professionals and training staff, among others. The third Scottish National Adaptation Plan (SNAP3) (Scottish Government, 2024c), sets out other on-going activities, including regulating the design and construction of new homes or buildings to avoid overheating; building resilience of school estates through the £2 billion Learning Estate Investment Programme (LEIP); and providing heat adaptation information for households and businesses on the Ready Scotland website.
Box 3.4 Opportunities for health and wellbeing in Scotland
A Public Health Scotland study on access to greenspace during the COVID-19 pandemic brought together surveys which registered between 70% and 90% agreement that greenspaces benefit mental health, regardless of income group (Public Health Scotland, 2022). But there are inequalities in accessibility of coastal blue space specifically. There is evidence from England that physical activity in green spaces increases with increasing temperature, and it’s reasonable to believe this will be the same in Scotland. The Scottish National Planning Framework (Scottish Government, 2024b), supports planning and development of ‘liveable places’ which aim to improve lifelong health and wellbeing and reduce health inequalities. One of four priorities for the National Transport Strategy (Transport Scotland, 2020) is to improve health and wellbeing by supporting people to choose active travel.
Evaluation of urgency score
Risk is Very High for current and all future time periods. Current risk has changed from High in CCRA3-IA TR to Very High due to new evidence from a comprehensive report; however, the confidence remains Low because the heat-related deaths in this report straddle between tens and over a hundred. There is Medium confidence for future periods due to limited evidence. Implemented adaptation is limited, and critical action is needed.
Table 3.5: Urgency scores for H1 Risks to people from heat for Scotland. Details of how the scores in this table were calculated are in the Methods Chapter.
| Scotland | |||||||||
| H1 | Risks to people from heat. | ||||||||
| Present | 2030 | 2050 | 2080 | ||||||
| Central | High | Central | High | Low | Central | High | |||
| No adaptation | VH • | VH • • | VH • • | VH • • | VH • • | VH • • | VH • • | VH • • | |
| With adaptation | VH • • | VH • • | VH • • | VH • • | VH • • | VH • • | VH • • | ||
| Urgency scores | CI | CAN | CAN | MAN | |||||
| Overall urgency score | CAN | ||||||||
3.2.1.5 Wales
Assessment of current magnitude of risk
Current risk is High. There are around 30 heat-related deaths per year (Gasparrini et al., 2022). A 2024 heat episode saw above-average levels for all-cause mortality, 999 calls for seizures, psychological and psychiatric A&E attendances, and GP consultations for heat stroke(Public Health Wales, 2025b, 2025a).
Assessment of future magnitude of risk
Future risk is assessed to be Very High. In the 2030s high scenario, assuming no population change, heat-related mortality is projected to be around 240 deaths a year (eight deaths per 100,000 people (Murage et al., 2024)). In the 2050s high scenario, this is projected to increase to 590 deaths a year (19 per 100,000 people). In the 2080s high scenario, Wales is projected to have 710 more annual heat deaths than in the near past (Jenkins et al., 2022). Urban areas exposed to direct sunlight could have a 4.5 °C increase in ‘peak heat stress’ (Huang et al., 2024).
Level of preparedness for risk
Public Health Wales provides hot weather public health guidance on their website to target groups, is improving climate-health surveillance (Public Health Wales, 2025b, 2025a), and is developing an Adverse Weather and Health Plan for Wales. Transport for Wales plans to develop heatwave communication plans for customers and colleagues and consider nature-based methods to prevent stations from overheating (Transport for Wales, 2023). The Welsh building regulations require overheating mitigation in new residential buildings. The Welsh Government is exploring extending requirements to existing buildings in their current Climate Change Adaptation Strategy (Welsh Government, 2024b). The Welsh Housing Quality Standard (Welsh Government, 2023b), requires social landlords to consider the impact of future overheating and install water butts where appropriate. Research has been commissioned to inform Business Wales on employee safety in high temperatures.
Box 3.5 Opportunities for health and wellbeing in Wales
The Green and Blue Spaces e-cohort was established to understand the impact of green and blue spaces on mental health and wellbeing in Wales (Geary et al., 2023). It used electronic health record data sources from 2008-2019, comprising nearly 3 million people. The study found that those with greater access to green space in their neighbourhood had lower odds of seeking help for common mental health disorders. This suggests living close to green and blue spaces is associated with positive impacts on mental health. Planning Policy Wales requires all levels of the planning process to develop Green Infrastructure Assessments to guide planning decisions (Welsh Government, 2024e). These assessments can identify opportunities for green/blue infrastructure development that may take advantage of any increased recreational opportunity and serve to reduce associated inequalities.
Evaluation of urgency score
Current confidence is Medium due to one robust study and new evidence from 2024 reports. We assess Very High risk across future periods, with Low to Medium confidence due to limited evidence. Fragmented policy actions and a lack of a national heatwave plan mean critical action is needed.
Table 3.6: Urgency scores for H1 Risks to people from heat for Wales. Details of how the scores in this table were calculated are in the Methods Chapter.
| Wales | |||||||||
| H1 | Risks to people from heat. | ||||||||
| Present | 2030 | 2050 | 2080 | ||||||
| Central | High | Central | High | Low | Central | High | |||
| No adaptation | H • • | VH • • | VH • • | VH • • | VH • • | VH • | VH • | VH • • | |
| With adaptation | VH • • | VH • • | VH • • | VH • • | VH • | VH • | VH • • | ||
| Urgency scores | MAN | CAN | CAN | FI | |||||
| Overall urgency score | CAN | ||||||||
3.2.2 Risks to people from extreme weather, excluding heat – H2
This risk covers extreme weather where there is evidence for an impact on human health and wellbeing in the UK. The risks covered are flooding, drought, storms (including wind, hail and thunder), wildfire, and cold. Heat is not included here but is covered separately in H1 due to its relevance to the UK. Water quality impacts on health related to flooding, including risks from exposure to pathogens, are covered in H4. While extreme low temperatures are considered within this risk (see Box 3.6), they are not used to inform the overall urgency scoring. This is because while cold is an important weather risk that will continue to shape winter mortality into the 2070s, it is not expected to increase with climate change in the ways that other weather extremes will.
Headlines
- There is more action needed to prevent future widespread health risks from extreme weather events (storms, drought, wildfire, flooding), with the largest health threat coming from flooding. Heat is addressed in H1, and has an even higher health burden.
- The most comprehensive evidence on current mental and physical health impacts comes from studies based on flood events, while the health risks of wildfire and drought are less well documented in the UK context.
- Negative health outcomes from future floods and droughts are expected to increase, as a larger percentage of the population become exposed over time, partly due to increased flood and drought risk.
- Cold hazards are treated separately. The negative health outcomes from cold are expected to continue until late in the century (2070s), and any reductions will not offset increased consequences of extreme heat. While heat risk will increase mortality and negative health impacts in summers, moderate cold weather will continue to pose significant health risks in winters.
- Across the UK, for all extreme weather types considered in H2, there is a lack of evidence on both mortality and morbidity rates, especially for future risks. New studies for health implications during extreme events, and in the months, years, and decades following are needed.
- Overall combined risks from extreme weather remain high throughout the UK, with new evidence since CCRA3-IA-TR confirming current risks and future potential trends and risks.
| Table 3.7: Urgency scores for H2 Risks to people from extreme weather, excluding heat. Details of how the scores in this table were calculated are in the Methods Chapter. | |||||||
| ID | Risk | Present | 2030 | 2050 | 2080 | Urgency | |
| H2 | Risks to people from extreme weather, excluding heat | UK | H • • • | H • • • | H • • • | H • • • | MAN |
| England | H • • • | H • • • | H • • • | H • • • | MAN | ||
| Northern Ireland | H • • • | H • • • | H • • • | H • • • | MAN | ||
| Scotland | H • • • | H • • • | H • • • | H • • • | MAN | ||
| Wales | H • • • | H • • • | H • • • | H • • • | MAN | ||
3.2.2.1 Evidence relevant to the entire United Kingdom
Current and future drivers of risk
Key climate drivers are increasingly influencing the risk, severity, and frequency of extreme weather in the UK, including hazards such as wildfire, cold, hail, ice, flooding (pluvial, fluvial, and coastal), storms, high winds, and drought. These weather risks are often interconnected: the initial hazard, such as flooding, can trigger wider disruptions to critical infrastructure, including transport, energy, and telecommunications systems, thereby amplifying societal impacts, including health risks. Moreover, individual extreme weather events create multiple hazards. The co-occurrence of wind and rainfall can significantly increase the scale and complexity of impacts compared to each hazard occurring in isolation (Manning et al., 2024). Interactions further compound risks: upstream, reduced water quality can impair water supply availability, while downstream, flooding and drought can pollute vital water sources used for drinking and recreation, leading to potential health risk (see I9). Additionally, wildfires can mobilise harmful chemicals, contaminating reservoirs and watercourses and having potential impacts on health (see I9) over and above the air quality-based risks. The impact of such hazards is socially patterned because of differential vulnerability associated for example with quality of housing and other protective factors or pre-existing ill health. The impact is also likely to be greater for people living with disability.
Assessment of current magnitude of risk
Current risk is assessed as High across the UK. This assessment suggests highest impacts from flood exposure, which is in the low hundreds of thousands of people affected, with additional risks coming from drought and other extreme events.
Flooding: This considers the risk from flooding to the health and wellbeing of individuals. The risk from flooding for buildings and communities is covered separately in BE2. Health impacts of flooding are both immediate (such as injuries, exposure to contaminated water, and disruption to healthcare services) and long-term (including persistent mental health issues like anxiety, depression, and post-traumatic stress). The magnitude for this risk remains High, in line with CCRA3-IA TR. Annual estimates of the numbers exposed to surface water or river and coastal flooding are in the low hundreds of thousands at present, with mental health consequences being potentially significant. New evidence since 2020, cited below, confirms significant flood risk to the UK and negative health consequences, supporting a confidence assessment of High based on studies with multiple lines of evidence and using multiple methods.
Increased UK flood risk from high river flows is in line with trends across northwest Europe in recent decades (Blöschl et al., 2019). There is evidence that the increased likelihood of flood events is due to both increased rainfall and deteriorating urban infrastructure (O’Donnell and Thorne, 2020), and that this amplifies health inequalities (Sayers, Penning-Rowsell and Horritt, 2018; Kew et al., 2024). Previously low-likelihood or unprecedented flood extremes are now assessed more likely (Kent et al., 2022; Kay et al., 2024).
The primary direct health effects linked with flooding in the UK are drowning, physical trauma, and infections from exposure to contaminated flood water (Parker, Mo and Goodman, 2022). The principal longer term health effects include mental health issues (such as anxiety and post-traumatic stress disorder), respiratory illness from damp and mould, and less likely and prevalent risks, such as those from rodent borne diseases (MHCLG, DHSC, and UKHSA, 2024). For mental health impacts, evidence suggests flood victims experience these outcomes 4-8.7 times more frequently than non-affected populations (Cruz et al., 2020). Other causes of negative health outcomes from flooding include community displacement, reduced opportunities for physical activity and sport (DCMS, 2025), risks during recovery such as carbon monoxide exposure due to use of indoor generators, property damage, dealing with administrative bureaucracy such as dealing with insurance claims, and the associated financial and mental burden of recovery (UKHSA, 2024d (HECC, chap.3)) Some of these aspects can be persistent over years because of home damage from damp and mould (Mulchandani et al., 2020), unrecoverable financial losses or more acute risks from disrupted access to health services in the aftermath of flood events (Dodd et al., 2024). Such impacts exacerbate health inequalities, meaning individuals with lower incomes, those without work, women and people with pre-existing medical conditions are all more susceptible to negative health outcomes.
Health impacts and associated personal health costs for affected populations correlate with flood depth, with a flood of up to 30cm depth costing £1,900 per adult and a flood of up to 1m costing approximately £4,100 per adult (2018 prices) (Environment Agency, 2021). These figures are per affected adult and encompass treatment expenses, including hospitalisation, general practitioner care, and medication, as well as work-related losses due to absenteeism (Mulchandani et al., 2020; Findlater et al., 2023). Drawing on these estimates, the costs of floods in terms of mental health are in the hundreds of millions of pounds annually.
Indirect impacts of flooding include increased pollution of land, water, and air (Talbot et al., 2018; Hanf et al., 2025), decreasing access to green space for residents, and disruption to ecosystems – which often displaces insects and animals which in turn increases human exposure to bites, stings, and potential infections (see H4). Given the increase in flood trends, the physical and mental health costs of floods are also shown to be increasing (Mulchandani et al., 2020; Findlater et al., 2023).
Drought: Drought-health effects in the UK include risks through both direct and indirect pathways. Direct pathways include limited water supply, loss of crops, damage to infrastructure and injury. Indirect pathways include ecosystem changes, such as change in breeding conditions for vectors, loss of biodiversity, supply chain disruption leading to potential food insecurity and malnutrition. All of these may have consequences for health. The Health Effects of Climate Change (HECC) in the UK report (UKHSA, 2024j (HECC chap.11)), highlights the UK’s vulnerability to prolonged hydrological droughts, though impacts vary geographically. The report also discusses the health impacts of meteorological, agricultural and socioeconomic droughts – all of which are likely to influence health in different ways. Attributing health effects to drought is challenging due to their slow onset, long exposure windows (potentially from seasons to years), and the influence of concurrent weather events such as heatwaves and wildfires. In addition, there is limited evidence in the UK specific context. What does exist is largely qualitative (Bryan et al., 2020; UKHSA, 2024j (HECC chap.11)). The strength of the quantified evidence of droughts on health is similar to CCRA3-IA TR, so the current risk magnitude does not change from Medium, and the confidence assessment is Low.
There is no evidence for the UK of direct mortality from physiological outcomes during droughts. The evidence is based around morbidity and mental health assessments. This includes through reduced water quality, reduced hygiene, food and air quality, algae blooms, transport disruption, vector borne disease shifts, and the impacts on health from fishery, crop, or livestock losses (Bryan et al., 2020; Barker et al., 2024). Negative impacts on wellbeing and increased risks of mental ill health in rural communities around periods of drought are a particular concern. A recent survey found that nine in ten farmers expressed having anxiety during recent periods of extreme weather in the UK context, with 60% responding that they were depressed and 6% very depressed (Energy & Climate Intelligence Unit, 2025).
Other extreme events: In addition to the extreme weather types already discussed, the UK experiences changes in health and wellbeing from storms, lightning, hail, thunderstorm asthma (see H3), wildfire burns, and respiratory impacts of wildfires (Mitchell et al., 2024). Extreme weather may lead to power outages, which impact on health, with those in vulnerable groups being particularly at risk (Cox, 2021).
Lightning in the UK poses a low annual fatality risk, with an average of two deaths per year, mostly associated with outdoor leisure and sports activities. Over the last two decades high winds and maximum gust speeds show a downward trend, while heavy rainfall shows a slight upward trend (Kendon et al., 2024). Both influence injuries and deaths, including those from road traffic accidents, through wind pressures, flying debris, and reduced visibility, especially during storms.
The effects of wildfire on human health and wellbeing are largely due to inhalation of particulate matter (see H3), pollutant impacts on skin conditions, burns, injuries, and longer-term mental wellbeing (Eisenman and Galway, 2022). There is limited evidence on fatalities and injuries from UK wildfires (UKHSA, 2024i (HECC chap.10)), although some studies exist on the health impacts through inhalation. Confidence is therefore rated as Medium as more insight and data are required.
Box 3.6 Cold
While the health impacts of cold are considered here, they are not used to inform the overall urgency scoring because they are not expected to increase with climate change in the ways that other weather risks will. However, they are also not expected to reduce significantly until later in the century (2070s) and any reductions will not offset increased health consequences of other weather risks.
Assessment of current magnitude of risk: There is robust evidence for thousands of deaths attributed to moderate and extreme cold each year, with estimates ranging between 13,400-28,000 depending on the years and methods used (Masselot et al., 2023; ONS, 2023; UKHSA, 2024e (HECC chap.2)). Though moderate and extreme cold episodes are decreasing, with fewer frost and ice days, it remains a Very High current risk with thousands of deaths from cold – the highest number of these is attributed to respiratory and cardiovascular diseases (HECC chap.2). Other health impacts include poor mental health, poor sleep quality, arthritic and mobility issues, allergies and dermatological issues, suppressed immune function, and pulmonary, respiratory and cardiovascular diseases (Janssen et al., 2023; Institute of Health Equity, 2024; UKHSA, 2024e (HECC chap.2)). Indirect effects include snow and ice disrupting healthcare services, fuel poverty, social isolation, poor mental health or carbon monoxide poisoning from poorly maintained or ventilated boilers, and cooking and heating appliances with combustion sources (UKHSA, 2025a (AWHP)).
These health impacts pose a disproportionate risk to young children and babies (from birth to six years of age), older people (65+), and those with pre-existing long-term mental and physical health conditions, such as cardiovascular or respiratory disease (Lee et al., 2022; Janssen et al., 2023; UKHSA, 2025a (AWHP)). Disabled people, UK minority ethnic groups, pregnant people, and low-income households, as well as those living in rented housing or experiencing homelessness, have also been identified as groups with greater risk of exposure to cold (Snell, Bevan and Thomson, 2015; Lee et al., 2022; UKHSA, 2025a (AWHP)).
Assessment of future magnitude of risk: Future risk for cold remains Very High magnitude for all nations for 2030 and 2050 time periods, when considering both moderate and extreme cold. The risk of extreme winter weather remains very high until 2070, and cold risk is expected to continue to lead to deaths in the 1000s until the end of the century. Extreme cold-related deaths are projected to increase for a period peaking in 2030 before declining by the mid-century (Murage et al., 2024; UKHSA, 2024e (HECC chap.2)). However, moderate and extreme cold combined is expected to remain a substantial mortality burden, and the total burden from moderate cold is projected to still exceed that from heat well into the 2070s (Masselot et al., 2023; UKHSA, 2024e (HECC chap.2)). Reductions in cold remain similar with limited realisation of these through to the end of the century and potential for any benefits during that time to be counteracted by an ageing population and increasingly wet conditions continuing to affect indoor environments (UKHSA, 2024e (HECC chap.2)). The modelled assessments for cold risk increasing out to 2070 are largely driven by population changes, particularly ageing.
Assessment of future magnitude of risk
The future risk is assessed as High across the UK. Highest impacts are from flood exposure which is in the low hundreds of thousands of people affected. While this number increases for future time periods, it never reaches the millions of people affected that would change the magnitude to Very High.
Flooding: Increased spatial and temporal resolution flood risk estimates for the UK have shown risks are likely to increase and expected annual damages are more responsive to climate than previously measured (Bates et al., 2023). Increases are expected in surface, ground, river, and coastal flooding. For instance, coastal flooding at the end of the century could lead to 120,000-160,000 properties potentially needing to be relocated, if the ‘hold the line’ policy is abandoned and with increased sea level and storminess associated with >2 °C warming (Sayers et al., 2022). Housing development on floodplains, poor land-use practices, and growing population pressures exacerbate the issue, ensuring the risk remains persistently high. Projected UK demographic changes, population growth and increasingly ageing populations will likely amplify the risk. Current estimates are of 6.1 million people exposed to flood risk that are projected to rise by 61% in 2050 under a 2 °C scenario, and 118% in a 4 °C scenario (UKHSA, 2024f (HECC chap.3)). The estimated annual numbers of people likely exposed to flooding in the future remain in the hundreds of thousands, with the economic costs of mental health being in the hundreds of millions. In terms of mortality, estimates suggest that for England there is a likely increase in the number of deaths from flooding in the 2050s from 18 per annum to 20 per annum (range 6 to 34) with no population growth or 29 per annum (range 8 to 49) with population growth (UKHSA, 2024f (HECC chap.3)).
Drought: Droughts are expected to become more frequent and intense due to rising global temperatures and shifting rainfall patterns, with risks expected to grow as climate change progresses (Arnell et al., 2021). The numbers of households impacted by water shortages will increase, with associated health impacts – particularly for vulnerable groups. Existing estimates on future risks to agricultural productivity associated with drought are projected to increase but are likely to remain at a Medium/High level across different scenarios (N6), with associated mental health risks for farmers. The health impacts of droughts are complex and often delayed, and there is emerging evidence for critical exposure periods, for instance changes in blood pressure are observed in adults decades after they were exposed, in utero, during hot dry conditions (Griffith et al, 2025; Lawson et al, 2008), although this relationship is complex. Those using private water supplies face particular challenges, including potential diminished bacteriological quality (Bryan et al., 2020; Public Health Wales, 2023e). Further detail on the risks to private water supplies can be found in the analysis for risk I9. Other significant changes include worsening air quality through wind-blown dust (such as Fen blows in East Anglia and stours in Scotland) (Bryan et al., 2020).
Other extreme events: Thunderstorms and lightning are poorly represented in conventional climate models, resulting in high uncertainty in their future trends (Finney et al., 2018; Kahraman et al., 2022). Longer term implications of most extreme weather conditions can increase psychological distress, worsen existing mental health conditions, and strain healthcare services (Green Alliance, 2024), or can have compounded health impacts from longer exposures, including from societal or economic changes, although much of this work is not quantified yet.
Level of preparedness for risk
The UK Government has made commitments to improve understanding of the risks of extreme weather and its impact on health and wellbeing, such as plans to conduct an annual survey of public perceptions of risk and preparedness, along with tracking socio-economic resilience (House of Commons Public Accounts Committee, 2024). The process of naming storms currently enhances the communication of extreme weather risks. The UK Government Resilience Framework (Cabinet Office, 2022) outlines a comprehensive approach to strengthening national resilience, including extreme weather, and the establishment of the National Situation Centre to monitor and manage risks. The Cabinet Office has also created a resilience directorate and established a senior-level Climate Resilience Board.
The UKHSA Adverse Weather and Health Plan (AWHP) for England, first published in April 2023, focuses on addressing the health effects of adverse weather and has undergone an equity review and impact assessment to evaluate its impact on various populations (UKHSA, 2025a (AWHP)). The AWHP consolidates guidance on health impacts from flooding, drought and cold (and heat), flagged by the UK National Risk Register (NRR) (Cabinet Office, 2025a), as well as thunderstorm asthma.
Much preparedness relies on local government and third sector action. The Severe Weather Emergency Protocol (SWEP) supports rough sleepers and people experiencing homelessness to receive emergency accommodation during periods of cold temperatures. Responses to cold weather risks come from across civil society and local government – as evidenced by the implementation of community-led warm spaces following high energy prices and cold weather in 2022. National retrofit programmes and fuel poverty support from government also improve preparedness for cold risks.
Assessment of the evidence base and evidence gaps
For the majority of extreme weather events in the UK, there is low consensus about the health consequences (Mitchell et al., 2024). There is High confidence on flood risks and their health consequences presently as the evidence comes from multiple sources using multiple methods and datasets. For other aspects of storms more generally, and for droughts, morbidity impacts remain underexplored and require further attention (UKHSA, 2024 (HECC)). Further research is also needed to understand how health inequalities intersect with climate change and extreme weather (Dodd et al., 2024).
3.2.2.2 England
Where sub-risks (flooding, drought, other extreme events) are not presented, no additional information was available and evidence for the UK (3.2.2.1) was used to assess risk.
Assessment of current magnitude of risk
Current risk is assessed as High for England. The highest impacts are from flood exposure, with additional risks coming from drought and other extreme events.
Flooding: Flood risk remains high across England, despite flood risk investments. Flood-related mortality is estimated to be 18 deaths per year on average (UKHSA, 2024f (HECC chap.3)). Wider morbidity consequences include impacts on respiratory and mental health. Mental health consequences of flooding have been identified as being particularly significant. Based on Environment Agency estimates of number of residential properties at high and medium risk of flooding (around 2.5 million for the current period), estimates of adults annually exposed to surface water or river and coastal flooding are in the low hundreds of thousands at present in England, giving an estimate for the scale of negative health impacts annually. The majority of the projected coastal flooding and inland flood risk increases are in England (Sayers et al., 2022; UKHSA, 2024f (HECC chap.3)).
Drought: The drought in Summer 2022 was the driest in England since 1935 (Met Office) and had a range of health-relevant impacts, including algal blooms, fish deaths, wildfires, low crop yields and impacts on livestock, transport disruption and water restrictions (Barker et al., 2024). There is increasing evidence of compound drought-flood risks in the literature (Parry et al., 2023). Quantification of the health impact is limited, though with the anticipated increase in water shortages there are likely to be increases in the risks to vulnerable groups in particular. Risks to the mental health of farmers due to drought will likely increase, depending on adaptation in the agricultural sector.
Other extreme events: The proportion of high and very high wildfire days has increased over the last 50 years in England, with a 50% increase in the number of high-risk days and a 240% increase in the number of very high-risk days (Thompson et al., 2025). No explicit analysis has linked that to health and wellbeing yet.
Assessment of future magnitude of risk
Future risk is assessed as High. Highest impacts will be from flood exposure, which is in the low hundreds of thousands of people affected, with additional risks coming from drought and other extreme events. While the number of people affected increases for future time periods, it never reaches the millions of people affected that would change the magnitude to Very High. The confidence is high, which is dominated by the confidence in the impacts of flooding on health.
Flooding: In the 2030s/2050s, the evidence suggests a relatively modest increase in deaths from flooding (covering inland, coastal and storm related flooding), to a range of 20 or 30 deaths per year depending on the climate scenario (UKHSA, 2024f (HECC chap.3)). However, wider health impacts from floods are expected to increase in line with increased exposure. The magnitude of the risk is assessed as High.
In the 2080s, the scale and scope of flood risk is likely to remain High. New future flood risk estimates coupled with insured economic costs for UK scenarios suggest estimates of future outcomes depend on global and UK mitigation efforts (Bates et al., 2023). Implementing actions that lead to climate futures with decarbonisation (e.g., implementing Paris Agreement) still means a projected 23-37% increase in flood economic losses by 2070. Current estimates of 6.1 million people living in flood prone areas rise by 118 percent in a 4°C scenario (UKHSA, 2024 (HECC chap.3)). This increased exposure may lead to a greater number of people impacted by flooding and adversely affecting their health and wellbeing. Annually, the numbers of people exposed to floods will be in the hundreds of thousands – with potential economic costs of mental health running into the hundreds of millions.
Drought: The risk of disruption to water supplies due to drought remains High under this scenario (see risk I9). There is limited additional evidence of the future level of risk to health and wellbeing compared to CCRA3-IA TR, despite increased understanding of the direct and indirect pathways from drought to health and wellbeing (Bryan et al., 2020; UKHSA, 2024j (HECC chap.11)).
In the 2050s, the risk of disruption to water supplies is considered High in the analysis for risk I9 across the different scenarios for England. For the 2080s, the magnitude of risks of supply disruption from drought to water supplies for England is very high, but the impact on health due to drought, including both direct and indirect pathways, has not been quantitatively estimated.
Level of preparedness for risk
The Flood Forecasting Centre (FFC) provides data, forecasts, and information to help plan for flood response. Ofwat oversees the climate resilience of water companies’ supply and wastewater systems in England and Wales. For England there are also health/heat, cold, and flood alerts in place.
Evaluation of urgency score
The risk magnitude is assessed as High for present and future scenarios with High confidence. The overall urgency is More action needed. Highest impacts will be from flood exposure, which is in the low hundreds of thousands of people affected, with additional risks coming from drought and other extreme events. While the number of people affected increases for future time periods, it never reaches the millions of people affected that would change the magnitude to Very High. The confidence is High, which is dominated by the confidence in the flooding impacts on health.
Table 3.8: Urgency scores for H2 Risks to people from extreme weather, excluding heat for England. Details of how the scores in this table were calculated are in the Methods Chapter.
| England | |||||||||
| H2 | Risks to people from extreme weather, excluding heat. | ||||||||
| Present | 2030 | 2050 | 2080 | ||||||
| Central | High | Central | High | Low | Central | High | |||
| No adaptation | H • • • | H • • • | H • • • | H • • • | H • • • | H • • • | H • • • | H • • • | |
| With adaptation | H • • • | H • • • | H • • • | H • • • | H • • • | H • • • | H • • • | ||
| Urgency scores | MAN | MAN | MAN | MAN | |||||
| Overall urgency score | MAN | ||||||||
3.2.2.3 Northern Ireland
Where sub-risks (flooding, drought, other extreme events) are not presented, no further data was available and evidence for the UK (3.2.2.1) was used to assess risk.
Assessment of current magnitude of risk
Current risk is assessed as High. Highest impacts are from flood exposure, which is in the tens of thousands of people affected annually based on calculations for England scaled to Northern Ireland population and data from the Northern Ireland Flood Risk Assessment (NIFRA), which estimates 45,000 properties at risk (Department for Infrastructure, 2018). Additional risks come from drought and other extreme events. While the number increases for future time periods, it never reaches the hundreds of thousands of people affected required to rank the risk as Very High. The confidence is High, reflecting the confidence in the estimates of the health impacts of flooding which dominate the magnitude scores. For other sub-risks the confidence would be Low.
The evidence for extreme weather impacts on health specifically for Northern Ireland is very sparse since CCRA3-IA TR. There is recent evidence relating to the use of private water wells, which is more common in Ireland than England, and these can be susceptible to contamination from flooding. Research from the Republic of Ireland may highlight shared risks in Northern Ireland. Musacchio et al. (2021) found that private well users in the Republic of Ireland are not well prepared for flood-related contamination, with underestimations of risk and a high percentage of people not undertaking proactive measures.
Assessment of future magnitude of risk
Future risk is assessed as High. While the number of impacts increases for future time periods, it never reaches the hundreds of thousands of people affected which would change the risk to Very High. The confidence is High, reflecting the confidence in the estimates of the health impacts of flooding which dominate the magnitude scores. For other sub-risks the confidence would be Low.
Level of preparedness for risk
The flood risk management plan is a requirement of The Water Environment Regulations (Northern Ireland) 2017 (DAERA, 2017), with one of the current (2021-2027) objectives being “to reduce the risk to life, health and wellbeing”. Northern Ireland Water have a climate change strategy (Northern Ireland Water, 2023) that includes improving sewer system informed by rainfall projects to reduce storm overflows, including keeping storm water out of sewers where feasible and flowing of rainwater flow with ponds and storage to avoid system being overwhelmed.
Evaluation of urgency score
The risk magnitude is assessed as High for present and future scenarios with High confidence. The overall urgency is More action needed. Highest impacts will be from flood exposure, with additional risks coming from drought and other extreme events. While the number of people affected increases for future time periods, it never reaches the thousands of people affected that would change the magnitude to Very High. The confidence is High, which is dominated by the confidence in the flooding impacts on health.
Table 3.9: Urgency scores for H2 Risks to people from extreme weather, excluding heat for Northern Ireland. Details of how the scores in this table were calculated are in the Methods Chapter.
| Northern Ireland | |||||||||
| H2 | Risks to people from extreme weather, excluding heat. | ||||||||
| Present | 2030 | 2050 | 2080 | ||||||
| Central | High | Central | High | Low | Central | High | |||
| No adaptation | H • • • | H • • • | H • • • | H • • • | H • • • | H • • • | H • • • | H • • • | |
| With adaptation | H • • • | H • • • | H • • • | H • • • | H • • • | H • • • | H • • • | ||
| Urgency scores | MAN | MAN | MAN | MAN | |||||
| Overall urgency score | MAN | ||||||||
3.2.2.4 Scotland
Where sub-risks (flooding, drought, other extreme events) are not presented, no further data were available and evidence for the UK (3.2.2.1) was used to assess risk.
Assessment of current magnitude of risk
Current risk is assessed as High. Highest impacts are from flood exposure, which is in the tens of thousands of people affected, with additional risks coming from drought and other extreme events.
Flooding: Only a small number of studies have focused on the impacts of flooding for people and communities in Scotland on both physical and mental health. A Centre of Expertise for Waters (CREW) (2024) study found long-term negative impacts on physical and emotional wellbeing of those affected by floods. Factors that make Scotland’s population at greater risk of health related impacts of flooding compared to UK average include; (i) aging population (the proportion of the population of pensionable age is expected to increase from about 20% to 25% by 2033); (ii) areas of greater deprivation and lower life expectancy than the rest of the UK; and (iii) a majority of the landmass classified as rural with a dispersed population (CREW 2024).
Drought: The risk of disruption to supplies in Scotland is considered to be high (see risk I9), and likely to have knock on health implications. A range of health impacts were identified in the Eden catchment in Scotland, including from loss of recreational activities in inland waters to “stours” (events with dust in the air) and impacts on sports injuries (Bryan et al., 2020). Based on expert judgement, and in line with CCRA3-IA TR, the overall health impacts of droughts in Scotland are likely to be Medium in this scenario.
Assessment of future magnitude of risk
Current risk is assessed as High. Highest impacts are from flood exposure, which is in the tens of thousands of people affected, with additional risks coming from drought and other extreme events. While the number of people affected increases for future time periods, it never reaches the hundreds of thousands of people which would change the risk to Very High. The confidence level is High, based on understanding of the health impacts of flooding and the dominance of this risk for the magnitude (the confidence in other sub-risks is low).
Flooding: The magnitude of flood risks is likely to remain High within Scotland. This is based on UK-wide scenarios of flood risk and the specific challenges of Scotland’s dispersed population, demographic profile of social disadvantage, and population health (CREW 2024). It also takes account of quoted projections of doubling of populations exposed to flood risk (Dow, 2025).
Drought: Following a similar justification as above, the magnitude of impacts for I9 (Risks to water supply and wastewater systems) in terms of disruption to water supply under this scenario are considered High under this scenario. Based on expert judgement, and following CCRA3-IA TR, the likely health impacts of droughts in Scotland in the 2030s are likely to be Medium in magnitude.
Level of preparedness for risk
The NHS Scotland Climate Emergency & Sustainability Strategy 2022-2026 (NHS Scotland, 2022) identifies the need to prepare and adapt to extreme weather. The NHS Scotland Standards for Organisational Resilience also requires that consideration is given to the non-traditional disaster response role of community healthcare settings. Plans should be in place to provide a healthcare response to people in the community following extreme weather events, especially those who are vulnerable, as part of the local multiagency recovery plan.
In 2024, Scotland published an adverse weather and health plan, which includes heat, cold, flooding and drought (Public Health Scotland, 2024). This aims to help reduce the burden of disease and health inequalities associated with adverse weather events in Scotland. It includes several action areas including: development of an epidemiology and surveillance system on adverse weather and health; scoping and potentially developing alert systems; development of advice and guidance; and public health messaging. The plan realises the need for a multi-agency, evidence-based approach in addressing the health risks associated with adverse weather in the Scottish context.
The Scottish Government’s 2024 National Flood Resilience Strategy outlines a comprehensive approach through 2045 and beyond (Scottish Government, 2024a). It highlights physical and mental health as a key outcome target in creating flood resilience. Scottish Water have a new climate change adaptation plan (Scottish Water, 2024). Water quality adaptations include completing a capability assessment of over 200 wastewater treatment works, followed by planning and implementing improvements.
Evaluation of urgency score
The risk magnitude is assessed as High for present and future scenarios with High confidence. The overall urgency is More action needed. Highest impacts will be from flood exposure, with additional risks coming from drought and other extreme events. While the number of people affected increases for future time periods, it never reaches the thousands of people affected that would change the magnitude to Very High. The confidence is High, which is dominated by the confidence in the flooding impacts on health.
Table 3.10: Urgency scores for H2 Risks to people from extreme weather, excluding heat for Scotland. Details of how the scores in this table were calculated are in the Methods Chapter.
| Scotland | |||||||||
| H2 | Risks to people from extreme weather, excluding heat. | ||||||||
| Present | 2030 | 2050 | 2080 | ||||||
| Central | High | Central | High | Low | Central | High | |||
| No adaptation | H • • • | H • • • | H • • • | H • • • | H • • • | H • • • | H • • • | H • • • | |
| With adaptation | H • • • | H • • • | H • • • | H • • • | H • • • | H • • • | H • • • | ||
| Urgency scores | MAN | MAN | MAN | MAN | |||||
| Overall urgency score | MAN | ||||||||
3.2.2.5 Wales
Where sub-risks (flooding, drought, other extreme events) are not presented, no additional data was available and evidence for the UK (3.2.2.1) was used to assess risk.
Assessment of current magnitude of risk
Current risk is assessed as High. Highest impacts are from flood exposure, which is in the tens of thousands of people affected, with additional risks coming from drought and other extreme events.
Flooding: Flooding from rivers is a current risk for approximately 243,000 people (Natural Resources Wales, 2023), and from the sea an estimated further 191,055 people are exposed. Nine areas in Wales are designated as National Flood Risk Areas due to the risks to health, economy, and the environment (Public Health Wales, 2023c (HIA D5.3)). Heavy downpours can also cause water ingress into coal tips (left over from mining operations) and subsequently lead to landslides, such as in 2020 and 2024, with targeted evidence that the 2020 Taylorstown landslide was linked to increased winter storms and more precipitation from climate change. This can cause mass causalities, as were seen in the 1966 Aberfan Disaster, and increased anxiety for communities living near the tips. Secondary affects can be from contaminated water for drinking or recreational use, and from health care disruption and displacement. It is mainly poorer communities who live near these tips (Public Health Wales, 2023a (HIA D5.7); The Guardian, 2024).
Drought: The magnitude of risk of low water supply is High (see I9 in this report). The health impacts on vulnerable communities may be reduced significantly by response measures (e.g., use of standpipes and other mechanisms to deliver water), but wider implications of drought on health exist (Bryan et al., 2020; UKHSA, 2024j (HECC chap.11)). For the Ebbw catchment, there have been reported impacts on recreation (particularly for people with disabilities), issues with bottled water quality for infants using formula milk, loss of livelihood, and mental health issues among farmers (Bryan et al., 2020).
Assessment of future magnitude of risk
Current risk is assessed as High. Highest impacts are from flood exposure, which is in the tens of thousands of people affected, with additional risks coming from drought and other extreme events. While the number affected increases for future time periods, it never reaches the hundreds of thousands of people affected which would change the risk to Very High. The confidence is High, associated with the level of confidence in the flooding-related health impacts (while confidence in the estimates of other sub-risks is low).
Flooding: The number of people exposed to frequent flooding is projected to rise significantly by 2050 (Natural Resources Wales, 2023).
Level of preparedness for risk
Wales uses the same Flood Forecasting Centre as England. Wales also has a Flood and Coastal Erosion Risk Management programme (Welsh Government, 2020) designed to protect people, property, and the environment from flooding and coastal erosion. This not only addresses physical flood risks but also examines the mental health impacts. The Water Health Partnership for Wales brings together public health professionals to work on issues across private and public drinking water supplies.
Key policy relevant measures to manage flood and coastal erosion risk in Wales include legislation like the Flood and Water Management Act 2010 (UK Government, 2010), strategic plans such as the National Strategy for Flood and Coastal Erosion Risk Management in Wales (Welsh Government, 2020), Shoreline Management Plans, and Planning Policy Wales (Welsh Government, 2024e). The latter includes additional tools like Technical Advice Notes (TANs) which guide national and local planning, development, and flood risk management to mitigate the impacts of flooding on communities and infrastructure.
Evaluation of urgency score
The risk magnitude is assessed as High for present and future scenarios with High confidence. The overall urgency is More action needed. Highest impacts will be from flood exposure, with additional risks coming from drought and other extreme events. While the number of people affected increases for future time periods, it never reaches the thousands of people affected that would change the magnitude to Very High. The confidence is High, which is dominated by the confidence in the flooding impacts on health.
Table 3.11: Urgency scores for H2 Risks to people from extreme weather, excluding heat for Wales. Details of how the scores in this table were calculated are in the Methods Chapter.
| Wales | |||||||||
| H2 | Risks to people from extreme weather, excluding heat. | ||||||||
| Present | 2030 | 2050 | 2080 | ||||||
| Central | High | Central | High | Low | Central | High | |||
| No adaptation | H • • • | H • • • | H • • • | H • • • | H • • • | H • • • | H • • • | H • • • | |
| With adaptation | H • • • | H • • • | H • • • | H • • • | H • • • | H • • • | H • • • | ||
| Urgency scores | MAN | MAN | MAN | MAN | |||||
| Overall urgency score | MAN | ||||||||
3.2.3 Risks to people from changes in air quality – H3
This section explores the current and future risks climate change poses to air quality. Air pollution and climate change are deeply connected in that (a) they are often caused by the same sources and (b) their effects on each other are bidirectional. For these reasons, they are most effectively tackled together. As a consequence, when assessing the risk to health caused by the impact of climate change on air quality (and what is being done to lessen this risk), the focus here is on the risk to health caused by air pollution as a whole, highlighting (where possible) the component climate change has, or will contribute in the future. Owing to the interconnectedness of these two environmental stressors, the climate component could feasibly be the consequence (or at least part) of primary/secondary emissions of air pollution.
Headlines
- While current and future risk to people from poor air quality (as a consequence of source emissions plus the additional contribution from climate change) has been scored as Very High (based primarily on mortality), there is low confidence over how much climate change contributes to this risk. This is due to a limited evidence base. This holds true for the UK as a whole, and for each of the devolved administrations.
- While phasing out the vast majority of fossil fuels and changes to agricultural practices will reduce emissions, changes in weather and climate patterns have the potential to exacerbate existing air quality risks in multiple ways.
- The future mix of air pollutants in the UK is unclear, as is how harmful they will be for human health. This is especially true when multiple air quality and weather stressors interact together.
- The risk magnitude has changed from High to Very High since CCRA3-IA-TR. This is primarily due to this report assessing total air pollution rather than just the climate component. However, it also reflects new evidence on health impacts of long-term exposure to very low levels of air pollution. In recognition of this, the revised World Health Organisation (WHO) air quality guidelines set more stringent limits.
| Table 3.12: Urgency scores for H3 Risks to people from changes in air quality. Details of how the scores in this table were calculated are in the Methods Chapter. | |||||||
| ID | Risk | Present | 2030 | 2050 | 2080 | Urgency | |
| H3 | Risks to people from changes in air quality | UK | VH • | VH • | VH • | VH • | CI |
| England | VH • | VH • | VH • | VH • | CI | ||
| Northern Ireland | VH • | VH • | VH • | VH • | CI | ||
| Scotland | VH • | VH • | VH • | VH • | CI | ||
| Wales | VH • | VH • | VH • | VH • | CI | ||
3.2.3.1 Evidence relevant to the entire United Kingdom
Current and future drivers of risk
Climate Hazards: High temperatures enhance the formation of ground-level ozone and particulate matter (PM). This occurs because of increased emissions of natural precursors (e.g., biogenic volatile organic compounds, ammonia) of air pollutants from vegetation and agricultural land, greater chemical reaction rates of air pollutants formed in the atmosphere and build-up of local emissions under stagnant meteorological conditions (Royal Society, 2021). Intense temperatures can lead to more wildfires that release large quantities of particularly toxic air pollutants such as PM, oxides of nitrogen (NOx), ozone and volatile organic compounds (VOCs) (UKHSA, 2024i (HECC chap.10)). Inside buildings, high temperatures increase the emission of VOCs from indoor sources, but may reduce the risk of mould (see BE5).
Droughts increase concentrations of PM through wind-driven emission of soil and dust, favour wildfires, and reduce the capacity of vegetation to uptake ozone because of stomatal closure (Royal Society, 2021). Heavy rainfall removes pollutants. Sea level rise and heavy rainfall increase the duration and frequency of flooding, which increases the risk of indoor mould growth (Pakdehi et al., 2025) (see BE5). Thunderstorms can rupture pollen and fungal spores (types of biological air pollutants), making them more respirable and this can trigger asthma epidemics among sensitised atopic asthmatic individuals (Elliot et al., 2021; UKHSA, 2022). A 2023 thunderstorm asthma event in London resulted in a 15-fold increase in paediatric emergency department presentations (Stewart, Mahesh and Mulvenna, 2024).
Strong winds can dilute and remove pollutants. Low wind speeds can trap and accumulate pollutants. Wind also serves to import human-made pollutants from mainland Europe, Saharan dust and volcanic ash from Iceland.
Outdoors, higher humidity can reduce ozone concentrations but promote secondary PM formation (i.e. PM formed in the atmosphere rather than directly emitted from a source). Indoors, rising humidity supports dampness and mould growth, particularly in poorly ventilated housing (see BE5). Atmospheric water vapour levels are high in the UK compared to other parts of the world, making UK homes particularly vulnerable.
Vulnerability: Air pollution does not affect everyone equally owing to differences in both physiological susceptibility and risk of exposure. Children face disproportionately high risks from air pollution, owing to their developing organ systems and higher respiratory rates (Sheridan, 2019; Defra, 2023). Pregnant people, and their unborn children face increased risks. PM exposure is linked to low birth weight and reduced lung function in childhood (Smith et al., 2017; Cai et al., 2020, p. 202; Chen et al., 2021; Deguen et al., 2021; RCOG, 2021; COMEAP, 2022). People’s exposure will be greater if they live, work or study in locations with high concentrations of air pollution, such as urban areas with high traffic density. Physiological susceptibility and greater risk of exposure can overlap. For example, people in lower socio-economic groups are more likely to (a) have pre-existing health conditions that constitute physiological susceptibility (Marmot et al., 2020) and (b) be exposed to poor in- and outdoor air quality because deprived neighbourhoods often have higher concentrations of air pollution (ONS, 2020a; Osborne et al., 2021; Williamson, Nunn and Pearce, 2021).
International elements: Pollutants generated outside the UK contribute to air pollution in the UK when weather patterns are favourable for this to occur. These include human made emissions from Europe (Stirling et al., 2020), smoke from wildfires (Augusto et al., 2020), large dust events from the Sahara (Vieno et al., 2016), and volcanic eruptions from Iceland (Elliot et al., 2010; Twigg et al., 2016).
Assessment of current magnitude of risk
The outdoor air pollutants with the greatest effect on the health of the UK population are PM, nitrogen dioxide (NO2) and ozone. The main sources of PM and NO2 are human made, with combustion from industry, transport and domestic sources playing a major role. The greatest effects are attributable to PM, measured as PM2.5 (particles smaller than 2.5 µm diameter) and PM10 (particles smaller than 10 µm diameter). Ozone is formed by chemical reactions in the atmosphere and concentrations are determined by complex relationships between NOx, VOCs and sunshine. The latest (2019) government estimates of the mortality burden of air pollution in the UK are 29,000–43,000 deaths (central estimate 36,000) per year for PM2.5 and NO2 combined (Mitsakou, Gowers and Exley, 2022). Reductions in pollutant concentrations since 2019 will have reduced these numbers towards a central estimate of approximately 30,000 deaths per year (Royal College of Physicians, 2025). Air pollution also increases the risk of cardiorespiratory disease, adverse pregnancy outcomes (Cai et al., 2020; RCOG, 2021)), diabetes (GBD 2019 Diabetes and Air Pollution Collaborators et al., 2022), and a decline in mental ability and an increase in dementia (COMEAP, 2022). Conversely, improvements in air quality are associated with improved health outcomes (Evangelopoulos et al., 2022). The health effects of outdoor air pollution can occur at very low concentrations (e.g., for PM2.5, as low as 4 µg/m3) (Brauer et al., 2019; Dominici et al., 2022; Stafoggia et al., 2022). In the UK, the risk of cardiovascular disease increases even at PM2.5 concentrations below 12-15 μg/m3 (i.e. below PM2.5 air quality standards across the UK) (Vanoli et al., 2024).
Over recent decades there has been a decreasing trend in the concentrations of PM2.5 and NO2 in the UK, reflecting considerable reductions in road vehicle exhaust emissions through improved technology and more electric vehicles. PM emissions from tyre, brake and road wear friction still occur, however, and may be more harmful to the lung than diesel exhaust PM (Parkin et al., 2025).
Indoor air quality is influenced by indoor sources such as smoke from solid fuels (e.g., wood, coal), NO2 from gas cooking and boilers, VOCs from consumer products and mould, as well as outdoor air pollution (see BE5). These air pollutants are associated with respiratory, cardiovascular, neurological and carcinogenic health effects (Guercio et al., 2021; eClinicalMedicine, 2022; Guercio, Doutsi and Exley, 2022; Halios et al., 2022; Clark et al., 2023, 2023; Delgado-Saborit et al., 2024). Ventilation is crucial in reducing concentrations of indoor pollutants (Petrou et al., 2022) (see BE5) but evidence suggests it is usually inadequate to ensure good air quality in the majority of UK homes (Dimitroulopoulou, 2012; Ministry of Housing, 2019).
Climate change can increase the risks to health from poor air quality by increasing concentrations of several air pollutants including PM, NO2 and ozone (See Figure 3.2 and 3.3.2.1) but a very limited evidence base prevents this climate component from being quantified. During heatwaves, an increase in outdoor ozone concentrations is observed (Scotland’s Environment, 2022; Defra, 2024a), and co-exposure to air pollutants (PM, ozone) and high temperatures may amplify individual health risks (Stafoggia et al., 2023; Zhang et al., 2024; Gao et al., 2025). The key emissions from wildfires include both PM and NO2, while ozone is also generated in the atmosphere during such events. PM from wildfire smoke may be more harmful to human health than non-fire PM, especially for cardiorespiratory health, owing to the presence of more fine and ultrafine particles and toxic gases (Ghetu et al., 2022; Alari et al., 2024). Associations exist between higher concentrations and earlier starts to the season of some pollen and fungal spores, and higher temperatures in the UK (Adams-Groom et al., 2022; Büntgen et al., 2022; Lam et al., 2024; UKHSA, 2024b (HECC chap.6)).

Figure 3.2: Summary of the impacts of climate change on air quality in the UK (Taken from Royal Society, 2021).
Assessment of future magnitude of risk
Outdoor concentrations of PM2.5 and NO2 are anticipated to further decline in coming decades in response to reduced emissions following changes to regulations, technology, urban planning, agricultural practices, and broader societal behaviour. Improvements in air quality will also inevitably begin to slow as many of the largest and most readily abated sources are addressed. An analysis of the impacts of interventions and policies relating to air quality indicate that compared to a 2018 baseline, by 2030 and 2050, exposure to PM2.5 will likely decrease by 24-30% and 28-36% respectively; NO2 exposure will decrease in 2030 and 2050 by 33-41% and 35-49% respectively (Macintyre et al., 2023b). Allowing for projected population growth, annual mortality attributable to long-term exposure to PM2.5 and NO2 is projected to decrease from 29,000-43,000 in 2018 to 18,887-32,342 in 2030 and 18,732-32,220 in 2050 (Macintyre et al., 2023b).
Concentrations of ozone in urban areas are likely to rise as local NOx emissions fall (Defra (AQEG) 2021; Grange et al., 2021). This is because pollutants such as NOx, that are more prevalent in urban areas, react with or “mop up” ozone and therefore reduce its concentration. Consequently, estimated emergency respiratory hospital admissions associated with short-term effects from ozone exposure under the business-as-usual emission policies are projected (including future population growth) to increase by 4.6% by 2030 and 11.7% by 2050 from a 2018 baseline of 60,488 (Macintyre et al., 2023a). Under a high emission scenario, for England, Scotland and Wales, and accounting for future population projections, estimated attributable deaths in 2050 associated with long-term exposure are 28,475 for PM2.5, 15,860 for NO2 and 13,101 for ozone (Fenech et al., 2021).
There is low confidence in the future magnitude of risk to health owing specifically to changes in outdoor air quality from climate change, owing to considerable uncertainty over the net impact of the broad mix of climate impacts (see Figure 3.2 and 3.3.2.1). Another uncertainty is that although we now know that there is no safe level of the current mix of anthropogenic-based PM2.5 that populations are currently exposed to, we do not yet know whether this will still be the case as sources (and possibly the toxicity) of pollutants shift in a changing environment. It is, however, likely that improvements in air quality (through reduced emissions) will be slowed or temporarily reversed by climate change, increasing risks to health once more.
Indoors, under both middle-of-the-road SSP2-4.5 and high emission SSP5-8.5 scenarios, limonene (a citrus scent used in many household products that can react with ozone to produce harmful air pollutants) and mould growth increase in indoor environments, while ozone rose under SSP5-8.5 (Zhao et al., 2024, 2025). Increased concentrations of limonene are attributed to a higher emission rate from furniture and building materials due to temperature increases (see BE5, 3.2.5). The risk of mould growth increases under high humidity. For some species of pollen and fungal spores, a warmer and wetter climate are expected to further increase growing seasons, level of production and potency (Kurganskiy et al., 2021; UKHSA, 2024i (HECC chap.10)).
Level of preparedness for risk
Air quality limit values are legal maximum concentrations for outdoor air pollutants. Limit values for PM, NO2 and ozone across England, Scotland, Wales, and Northern Ireland are broadly aligned but not identical, due to devolved powers and differing policy approaches. No national government has, however, aligned their air quality standards with the WHO’s 2021 air quality guidelines. The Daily Air Quality Index (DAQI) is the national alert system that provides information to the public about outdoor air pollution levels in local areas as well as recommended actions and health advice (Defra, 2025d). However, it is recognised that Defra air pollution forecasts are typically county-to-regional in geographic scope and lack street or postcode-level details that may help support direct behavioural adjustments; for example, providing guidance on the avoidance of hotspots in cities or by roads. Policy relating to indoor air pollutants crosses the interfaces of multiple government departments and agencies, leading to a fragmented regulatory framework and a lack of ownership.
Local initiatives to reduce air pollution integrate actions that include transport (e.g., clean air zones, low traffic neighbourhoods), urban planning and design, reducing pollution around schools and monitoring (DHSC CMO, 2022; Greater London Authority, 2025). UK100, a network of councils across the UK that supports a local-led rapid transition to Net Zero and Clean Air (UK100, 2023).
Non-governmental adaptation occurs through the activities of networks and charitable organisations. This includes Asthma & Lung UK, Mums for Lungs, Global Action Plan. There is guidance for local authorities on integrating action on air quality and climate change by the Institution of Environmental Sciences (2024).
Assessment of the evidence base and evidence gaps
Information is missing on the extent to which a changing climate will affect the risk to health caused by poor air quality, specifically: health effects of interactions between air pollutants and a changing climate; harm to health of a future pollutant mix under the influence of climate change; how climate change-driven behaviours could modify personal exposure to air pollution (UKHSA, 2024g (HECC chap.4)); effects of home decarbonisation (in new buildings and retrofitted infrastructure) on concentrations of indoor air pollutants and consequential health benefits (UKHSA, 2024a (HECC chap.5)); an understanding of the composition of UK wildfire smoke and its short-term and long-term impact on mortality and morbidity (UKHSA, 2024i (HECC chap.10)).
3.2.3.2 England
Assessment of current magnitude of risk
The current magnitude of risk caused by total air pollution (i.e. source emissions plus the additional contribution from climate change) is Very High. This is based on a total of 26,000 to 38,000 annual deaths (46-68 deaths per 100,000) attributed to outdoor anthropogenic air pollution (Mitsakou, Gowers and Exley, 2022). The confidence of this magnitude score is Low for this risk to health, owing to uncertainty in changes in air quality from climate change (due to a limited evidence base).
Assessment of future magnitude of risk
There is a particular risk of wildfires over the moorland regions of northern England, affecting surrounding regions including population centres. Southeast England is more likely to be affected by heatwaves and droughts and with that, greater exposure to pollutants (particularly PM and ozone) from UK sources and inflow from Europe (Royal Society, 2021). An analysis of air quality, ambient temperatures, and climate change adaptation plans in 30 UK cities (covering around 17.3 million of the UK population and including the capitals of England, Northern Ireland, Scotland and Wales) found that London and Cambridge exhibit the highest risk of both extreme temperature and air pollution (Chauhan et al., 2025). The air of western coastal regions may be cleansed by stronger westerly flow and greater wintertime rainfall.
In a 2030s, central warming scenario, the risk caused by total air pollution (i.e. source emissions plus the additional contribution from climate change) without adaptation (i.e. air pollution emission policies) is Very High. This is based on a total of 28,701 to 41,948 annual deaths (46-68 deaths per 100,000) attributed to outdoor air pollution arising from anthropogenic emissions. Number of deaths calculated by extrapolating, using the 10.39% increase in population from 2019 to 2035 (ONS, 2020b, 2025), the mortality burden in 2019 (Mitsakou, Gowers and Exley, 2022) to that in 2035. The risk with adaptation is Very High. This is based on a total of 15,284-26,002 deaths (25-42 deaths per 100,000) attributable to the effects of long-term exposure to PM2.5 & NO2 (Macintyre et al., 2023b) and 50,101 annual total of daily emergency respiratory admissions associated with short-term ozone exposure (Macintyre et al., 2023a) under current UK & European emission policies. There is however low confidence (due to a limited evidence base) in this risk to health owing to changes in air quality from climate change, and this is the case with and without adaptation.
In a 2050s central warming scenario the risk caused by total air pollution (i.e. source emissions plus the additional contribution from climate change) without adaptation is Very High. This is based on a total of 30,830-45,060 annual deaths (46-68 deaths per 100,000) attributed to outdoor air pollution arising from anthropogenic emissions. Number of deaths calculated by extrapolating, using the 18.58% increase in population from 2019 to 2055 (ONS, 2020b, 2025), the mortality burden in 2019 (Mitsakou, Gowers and Exley, 2022) to that in 2055. A total of 14,251-24,400 deaths (22-37 deaths per 100,000) attributable to the effects of long-term exposure to PM2.5 & NO2 (Macintyre et al., 2023b) and 52,319 annual total of daily emergency respiratory admissions associated with short-term ozone exposure (Macintyre et al., 2023a) under current UK & European emission policies (no account of climate change). There is however low confidence (due to a limited evidence base) in this risk to health owing to changes in air quality from climate change, and this is the case with and without adaptation.
In a 2080s, central warming scenario, the risk caused by total air pollution (i.e. source emissions plus the additional contribution from climate change) without adaptation is Very High. This is based on a total of 32,479-47,470 annual deaths (46-68 deaths per 100,000) attributed to outdoor air pollution arising from anthropogenic emissions. Number of deaths calculated by extrapolating, using the 24.92% increase in population from 2019 to 2085 (ONS, 2020b, 2025), the mortality burden in 2019 (Mitsakou, Gowers and Exley, 2022) to that in 2085. In the absence of projections, the prediction of risk with adaptation involves expert judgment where there is a high level of agreement. While air quality in the late century will substantially benefit from the phasing out of the vast majority of fossil fuels and changes to agricultural practices, events such as heatwaves and drought will worsen outdoor air quality and, in turn, the quality of indoor air (see BE5). Events such as sea level rise, heavy rainfall and thunderstorms will bring about risk of damp buildings, increased growth of indoor mould and increase asthma epidemics among sensitised atopic asthmatic individuals (see BE5). Without response planning, particularly within urban areas, there is potential for the risk to remain Very High. There is, however, low confidence (due to a limited evidence base) in this risk to health owing to changes in air quality from climate change, and this is the case with and without adaptation.
Level of preparedness for risk
Regarding the reduction of air pollutant emissions, there are two air quality targets for PM2.5 in England: a legal target to meeting an annual average 10 µg/m3 limit value by 2040; and an interim target of 12 µg/m3 by the end of January 2028 (Defra, 2019 (Clean Air Strategy); HM Government, 2021 (Environment Act)). Additional anthropogenic emission adaptation to that currently in place is needed to meet the target limit value of PM2.5 of 10 µg/m3 (Defra, 2022).
Approved Document F includes a methodology that helps maintain adequate levels of ventilation when energy efficiency measures are installed (MHCLG, 2022). The Air Quality (Domestic Solid Fuels Standards) (England) Regulations 2020 (HM Government, 2020) banned the sale of traditional house coal completely in England from May 2023 (although ‘smokeless’ fuels are still permitted) and introduced regulation of the sale of wood fuel to control its moisture content in order to reduce PM2.5 emissions when burned.
With regard to reduction in a worsening of air quality owing to climate change, a Centre for Climate and Health Security has been established within the UKHSA to protect health in the context of a changing climate. Activities include: systematic review on the evidence for the health effects due to exposure to short-term ozone being modified by increases in temperature (UKHSA, 2024a (HECC chap.5)); planning, response, and awareness of wildfires as well as strengthening the evidence base on wildfires and health (UKHSA, 2024g (HECC chap.4)), research into aeroallergens (UKHSA, 2024b (HECC chap.6)) and publication of guidance on damp and mould for rented housing providers (MHCLG, DHSC, and UKHSA, 2024).
Evaluation of urgency score
Due to the Very High projected magnitude for the risk caused by total air pollution (i.e., source emissions plus the additional contribution from climate change) but Low confidence (due to a limited evidence base) in the size of the contribution from the climate change component, this risk has been scored as Critical investigation.
N.B. The High magnitude score for a low warming 2080 scenario is based on expert opinion: improved air quality because of (a) the phasing out of the vast majority of fossil fuels and improved agricultural practices and (b) lower warming outcomes (e.g., heatwaves, sea level rises).
Table 3.13: Urgency scores for H3 Risks to people from changes in air quality for England. Details of how the scores in this table were calculated are in the Methods Chapter.
| England | |||||||||
| H3 | Risks to people from changes in air quality. | ||||||||
| Present | 2030 | 2050 | 2080 | ||||||
| Central | High | Central | High | Low | Central | High | |||
| No adaptation | VH • | VH • | VH • | VH • | VH • | VH • | VH • | VH • | |
| With adaptation | VH • | VH • | VH • | VH • | H • | VH • | VH • | ||
| Urgency scores | CI | CI | CI | FI | |||||
| Overall urgency score | CI | ||||||||
3.2.3.3 Northern Ireland
Assessment of current magnitude of risk
The current magnitude of risk caused by total air pollution (i.e. source emissions plus the additional contribution from climate change) is Very High. This is based on a total of 470 to 730 annual deaths (25-39 deaths per 100,000) attributed to outdoor anthropogenic air pollution (Mitsakou, Gowers and Exley, 2022). The confidence of this magnitude score is Low for this risk to health, owing to uncertainty in changes in air quality from climate change (due to a limited evidence base).
Assessment of future magnitude of risk
In a 2030s central warming scenario, the risk caused by total air pollution (i.e. source emissions plus the additional contribution from climate change) without adaptation (i.e. air pollution emission policies) is Very High. This is based on a total of 484 to 752 annual deaths (25-39 deaths per 100,000) attributed to outdoor air pollution arising from anthropogenic emissions. Number of deaths calculated by extrapolating, using the 2.97% increase in population from 2019 to 2035 (ONS, 2020b, 2025), the mortality burden in 2019 (Mitsakou, Gowers and Exley, 2022) to that in 2035. The risk with adaptation is Very High. This is based on a total of 275-538 deaths (14-28 deaths per 100,000) attributable to the effects of long-term exposure to PM2.5 & NO2 (Macintyre et al., 2023b) and 3,269 annual total of daily emergency respiratory admissions associated with short-term ozone exposure (Macintyre et al., 2023a) under current UK & European emission policies (no account of climate change). There is however Low confidence (due to a limited evidence base) in the risk to health owing specifically to changes in air quality from climate change, and this is the case without and with adaptation.
In a 2050s, central warming scenario, the risk caused by total air pollution (i.e. source emissions plus the additional contribution from climate change) without adaptation is Very High. This is based on a total of 473 to 735 annual deaths (25-39 deaths per 100,000) attributed to outdoor air pollution arising from anthropogenic emissions. Number of deaths calculated by extrapolating, using the 0.7% increase in population from 2019 to 2035 (ONS, 2020b, 2025), the mortality burden in 2019 (Mitsakou, Gowers and Exley, 2022) to that in 2055. The risk with adaptation is Very High based on a total of 263-507 deaths (14-27 deaths per 100,000) attributable to the effects of long-term exposure to PM2.5 & NO2 (Macintyre et al., 2023b) and 3,270 annual total of daily emergency respiratory admissions associated with short-term ozone exposure (Macintyre et al., 2023a) under current UK & European emission policies (no account of climate change). There is however Low confidence (due to a limited evidence base) in the risk to health owing specifically to changes in air quality from climate change, and this is the case with and without adaptation.
In a 2080s, central warming scenario, the risk caused by total air pollution (i.e. source emissions plus the additional contribution from climate change) without adaptation is Very High. This is based on a total of 422 to 655 annual deaths (25-39 deaths per 100,000) attributed to outdoor air pollution arising from anthropogenic emissions. Number of deaths calculated by extrapolating, using the 10.23% decrease in population from 2019 to 2085 (ONS, 2020b, 2025), the mortality burden in 2019 (Mitsakou, Gowers and Exley, 2022) to that in 2085. In the absence of projections, the prediction of risk with adaptation involves expert judgment where there is a high level of agreement: while air quality in the late century will substantially benefit from the phasing out of the vast majority of fossil fuels and changes to agricultural practices, increases in heatwaves and drought will worsen outdoor air quality and, in turn, the quality of indoor air (see BE5). Events such as sea level rise, heavy rainfall and thunderstorms will bring about risk of damp buildings, increased growth of indoor mould and increase asthma epidemics among sensitised atopic asthmatic individuals (see BE5). Without response planning, particularly within urban areas, there is potential for the risk to remain Very High. There is however Low confidence (due to a limited evidence base) in the risk to health owing specifically to changes in air quality from climate change, and this is the case with and without adaptation.
Level of preparedness for risk
The first Clean Air Strategy for Northern Ireland (due to be published in 2025) cites the need for integrated and coordinated strategies on air quality and carbon reduction to be coordinated (DAERA, 2020); Environmental Improvement Plan for Northern Ireland (DAERA, 2024a) ; Draft Green Growth Strategy for Northern Ireland (DAERA, 2021). Climate Northern Ireland have an online tool kit to support the first phase of climate adaptation planning in local councils (Climate Northern Ireland, 2025).
Evaluation of urgency score
Due to the Very High projected magnitude for the risk caused by total air pollution (i.e. source emissions plus the additional contribution from climate change) but Low confidence (due to a limited evidence base) in the size of the contribution from the climate change component, this risk has been scored as Critical investigation.
N.B. The High magnitude score for a low warming 2080 scenario is based on expert opinion: improved air quality because of (a) the phasing out of the vast majority of fossil fuels and improved agricultural practices and (b) lower warming outcomes (e.g., heatwaves, sea level rises).
Table 3.14: Urgency scores for H3 Risks to people from changes in air quality for Northern Ireland. Details of how the scores in this table were calculated are in the Methods Chapter.
| Northern Ireland | |||||||||
| H3 | Risks to people from changes in air quality. | ||||||||
| Present | 2030 | 2050 | 2080 | ||||||
| Central | High | Central | High | Low | Central | High | |||
| No adaptation | VH • | VH • | VH • | VH • | VH • | VH • | VH • | VH • | |
| With adaptation | VH • | VH • | VH • | VH • | H • | VH • | VH • | ||
| Urgency scores | CI | CI | CI | FI | |||||
| Overall urgency score | CI | ||||||||
3.2.3.4 Scotland
Assessment of current magnitude of risk
The current magnitude of risk caused by total air pollution (i.e. source emissions plus the additional contribution from climate change) is Very High. This is based on a total of 1,800 to 2,700 annual deaths (33-49 deaths per 100,000) attributed to outdoor anthropogenic air pollution (Mitsakou, Gowers and Exley, 2022). The confidence of this magnitude score is Low for this risk to health, owing to uncertainty in changes in air quality from climate change (due to a limited evidence base).
Assessment of future magnitude of risk
There is a particular risk of wildfires over the moorland regions of Scotland, affecting surrounding regions including population centres. The air of western coastal regions may be cleansed by stronger westerly winds and greater wintertime rainfall (Royal Society, 2021).
In a 2030s central warming scenario, the risk caused by total air pollution (i.e. source emissions plus the additional contribution from climate change) without adaptation (i.e. air pollution emission policies) is Very High based on a total of 1,880 to 2,820 annual deaths (25-39 deaths per 100,000) attributed to outdoor air pollution arising from anthropogenic emissions. Number of deaths calculated by extrapolating, using the 4.44% increase in population from 2019 to 2035 (ONS, 2020b, 2025), the mortality burden in 2019 (Mitsakou, Gowers and Exley, 2022) to that in 2035. The risk with adaptation is Very High based on a total of 1131-1898 deaths (20-33 per 100,000) attributable to the effects of long-term exposure to PM2.5 & NO2 (Macintyre et al., 2023b) and 8,644 annual total of daily emergency respiratory admissions associated with short-term ozone exposure (Macintyre et al., 2023a) under current UK & European emission policies (no account of climate change). There is however Low confidence (due to a limited evidence base) in the risk to health owing specifically to changes in air quality from climate change, and this is the case without and with adaptation.
In a 2050s, central warming scenario, the risk caused by total air pollution (i.e. source emissions plus the additional contribution from climate change) without adaptation is Very High based on a total of 1,905 to 2,857 annual deaths (25-39 deaths per 100,000) attributed to outdoor air pollution arising from anthropogenic emissions. Number of deaths calculated by extrapolating, using the 5.83% increase in population from 2019 to 2055 (ONS, 2020b, 2025), the mortality burden in 2019 (Mitsakou, Gowers and Exley, 2022) to that in 2035. The risk with adaptation is Very High based on a total of 1075-1805 deaths (19-31 per 100,000) attributable to the effects of long-term exposure to PM2.5 & NO2 (Macintyre et al., 2023b) and 8,644 annual total of daily emergency respiratory admissions associated with short-term ozone exposure (Macintyre et al., 2023a) under current UK & European emission policies (no account of climate change). There is, however, Low confidence (due to a limited evidence base) in the risk to health owing specifically to changes in air quality from climate change, and this is the case with and without adaptation.
In a 2080s, central warming scenario, the risk caused by total air pollution (i.e. source emissions plus the additional contribution from climate change) without adaptation is Very High based on a total of 1,893 to 2,839 annual deaths (25-39 deaths per 100,000) attributed to outdoor air pollution arising from anthropogenic emissions. Number of deaths calculated by extrapolating, using the 5.14% increase in population from 2019 to 2055 (ONS, 2020b, 2025), the mortality burden in 2019 (Mitsakou, Gowers and Exley, 2022) to that in 2085. In the absence of projections the prediction of risk with adaptation involves expert judgment where there is a high level of agreement: while air quality in the late century will substantially benefit from the phasing out of the vast majority of fossil fuels and changes to agricultural practices, increases in heatwaves and drought will worsen outdoor air quality and in turn, the quality of indoor air (see BE5). Events such as sea level rise, heavy rainfall and thunderstorms will bring about risk of damp buildings, increased growth of indoor mould and increase asthma epidemics among sensitised atopic asthmatic individuals (see BE5). Without response planning, particularly within urban areas, there is potential for the risk to remain Very High. There is, however, Low confidence (due to a limited evidence base) in the risk to health owing specifically to changes in air quality from climate change, and this is the case with and without adaptation.
Level of preparedness for risk
Scotland has air quality target for PM2.5 of 10µg m3. Cleaner Air for Scotland 2 (Scottish Government, 2021) includes an ‘Integrated Policy’ in which it states that strategies, policies and plans being developed by central government for climate change mitigation and adaptation should be closely coordinated and aligned with those for air quality to maximise co-benefits. Air quality is included in the Climate Ready School Grounds guidance (Architecture & Design Scotland, 2023). The New Build Heat Standard designed to reduce emissions from domestic heating was heavily scaled back following publication (Scottish Government, 2025a).
Evaluation of urgency score
Due to the Very High projected magnitude for the risk caused by total air pollution (i.e. source emissions plus the additional contribution from climate change) but Low confidence (due to a limited evidence base) in the size of the contribution from the climate change component, this risk has been scored as Critical investigation.
N.B. The High magnitude score for a low warming 2080 scenario is based on expert opinion: improved air quality because of (a) the phasing out of the vast majority of fossil fuels and improved agricultural practices and (b) lower warming outcomes (e.g., heatwaves, sea level rises).
Table 3.15: Urgency scores for H3 Risks to people from changes in air quality for Scotland. Details of how the scores in this table were calculated are in the Methods Chapter.
| Scotland | |||||||||
| H3 | Risks to people from changes in air quality. | ||||||||
| Present | 2030 | 2050 | 2080 | ||||||
| Central | High | Central | High | Low | Central | High | |||
| No adaptation | VH • | VH • | VH • | VH • | VH • | VH • | VH • | VH • | |
| With adaptation | VH • | VH • | VH • | VH • | H • | VH • | VH • | ||
| Urgency scores | CI | CI | CI | FI | |||||
| Overall urgency score | CI | ||||||||
3.2.3.5 Wales
Assessment of current magnitude of risk
The current magnitude of risk caused by total air pollution (i.e. source emissions plus the additional contribution from climate change) is Very High based on a total of 1,200 to 2,000 annual deaths (38-63 per 100,000) attributed to outdoor anthropogenic air pollution (Mitsakou, Gowers and Exley, 2022). The confidence of this magnitude score is Low for this risk to health, owing to uncertainty in changes in air quality from climate change (due to a limited evidence base).
Assessment of future magnitude of risk
There is a particular risk of wildfires over the moorland regions of Wales, affecting surrounding regions including population centres.
In a 2030s, central warming scenario, the risk caused by total air pollution (i.e. source emissions plus the additional contribution from climate change) without adaptation (i.e. air pollution emission policies) is Very High based on a total of 1,275 to 2,124 annual deaths (38-63 per 100,000) attributed to outdoor air pollution arising from anthropogenic emissions. Number of deaths calculated by extrapolating, using the 6.22% increase in population from 2019 to 2035 (ONS, 2020b, 2025), the mortality burden in 2019 (Mitsakou, Gowers and Exley, 2022) to that in 2035. The risk with adaptation is Very High based on a total of 759-1442 (23-43 per 100,000) deaths attributable to the effects of long-term exposure to PM2.5 & NO2 (Macintyre et al., 2023b) and 3,480 annual total of daily emergency respiratory admissions associated with short-term ozone exposure (Macintyre et al., 2023a) under current UK & European emission policies (no account of climate change). There is, however, Low confidence (due to a limited evidence base) in the risk to health owing specifically to changes in air quality from climate change, and this is the case with and without adaptation.
In a 2050s, central warming scenario, the risk caused by total air pollution (i.e. source emissions plus the additional contribution from climate change) without adaptation is Very High based on a total of 1,334 to 2,224 annual deaths (38-63 per 100,000) attributed to outdoor air pollution arising from anthropogenic emissions. Number of deaths calculated by extrapolating, using the 11.2% increase in population from 2019 to 2055 (ONS, 2020b, 2025), the mortality burden in 2019 (Mitsakou, Gowers and Exley, 2022) to that in 2055. The risk with adaptation is Very High (VH) based on a total of 714-1348 deaths (20-38 per 100,000) attributable to the effects of long-term exposure to PM2.5 & NO2 (Macintyre et al., 2023b) and 3,556 annual total of daily emergency respiratory admissions associated with short-term ozone exposure (Macintyre et al., 2023a) under current UK & European emission policies (no account of climate change). There is, however, Low confidence (due to a limited evidence base) in the risk to health owing specifically to changes in air quality from climate change, and this is the case without and with adaptation.
In a 2080s, central warming scenario, the risk caused by total air pollution (i.e. source emissions plus the additional contribution from climate change) without adaptation is Very High based on a total of 1,354 to 2,258 annual deaths (38-63 per 100,000) attributed to outdoor air pollution arising from anthropogenic emissions. Number of deaths calculated by extrapolating, using the 12.88% increase in population from 2019 to 2085 (ONS, 2020b, 2025), the mortality burden in 2019 (Mitsakou, Gowers and Exley, 2022) to that in 2085. In the absence of projections the prediction of risk with adaptation involves expert judgment where there is a high level of agreement: while air quality in the late century will substantially benefit from the phasing out of the vast majority of fossil fuels and changes to agricultural practices, increases in heatwaves and drought will worsen outdoor air quality and in turn, the quality of indoor air (see BE5). Events such as sea level rise, heavy rainfall and thunderstorms will bring about risk of damp buildings, increased growth of indoor mould and increase asthma epidemics among sensitised atopic asthmatic individuals (see BE5). Without response planning, particularly within urban areas, there is potential for the risk to remain Very High. There is, however, Low confidence (due to a limited evidence base) in the risk to health owing specifically to changes in air quality from climate change, and this is the case without and with adaptation.
Level of preparedness for risk
The Environment (Air Quality and Soundscapes) (Wales) Act (2024) aims to establish a PM2.5 target by February 2027 (Welsh Government, 2024c). There are actions to ensure that a risk from climate change is considered in future policy development to improve air quality (Welsh Government, 2024b). Update to the Building Regulations part F (ventilation) addresses overheating and indoor air quality (Welsh Government, 2025a).
Evaluation of urgency score
Due to the Very High projected magnitude for the risk caused by total air pollution (i.e. source emissions plus the additional contribution from climate change) but Low confidence (due to a limited evidence base) in the size of the contribution from the climate change component, this risk has been scored as Critical investigation.
N.B. The High magnitude score for a low warming 2080 scenario is based on expert opinion: improved air quality because of (a) the phasing out of the vast majority of fossil fuels and improved agricultural practices and (b) lower warming outcomes (e.g., heatwaves, sea level rises).
Table 3.16: Urgency scores for H3 Risks to people from changes in air quality for Wales. Details of how the scores in this table were calculated are in the Methods Chapter.
| Wales | |||||||||
| H3 | Risks to people from changes in air quality. | ||||||||
| Present | 2030 | 2050 | 2080 | ||||||
| Central | High | Central | High | Low | Central | High | |||
| No adaptation | VH • | VH • | VH • | VH • | VH • | VH • | VH • | VH • | |
| With adaptation | VH • | VH • | VH • | VH • | H • | VH • | VH • | ||
| Urgency scores | CI | CI | CI | FI | |||||
| Overall urgency score | CI | ||||||||
3.2.4 Risks to people from climate-sensitive infectious diseases – H4
Climate-sensitive infectious diseases are diseases caused by pathogens (such as bacteria, viruses, and parasites) whose transmission, incidence or spatial distribution is influenced by weather patterns or climate conditions. Climate change is influencing the risk of transmission of many of these diseases. Climate-sensitive infections have different transmission pathways that can be useful for understanding policy and adaptation solutions, including but not limited to 1) vector-borne (infections caused by parasites, viruses and bacteria which are transmitted by blood-feeding arthropod vectors), 2) water- and food-borne and 3) air-borne. In our summaries, we use these categorisations, but in the main evidence base we sort by individual pathogen, as many of them have multiple routes of transmission (UKHSA, 2024c (HECC chap.7)). Whilst other health-related issues linked to climate-sensitive diseases, such as those from antimicrobial resistance (AMR), are discussed in this risk, only the risk to people from climate-sensitive infectious diseases is included in the urgency scores.
Headlines
- West Nile virus and tick-borne encephalitis have recently been detected in the UK for the first time. Outbreaks of dengue and chikungunya are now being reported in neighbouring countries, such as France and Spain.
- There is strong evidence for the impact of weather and climate on some pathogens such as Campylobacter, Salmonella and Vibrio, but for many others the evidence is currently lacking. Enhanced pathogen monitoring is the first step to strengthening this evidence and helping identify adaptation strategies.
- There is a lack of modelling studies projecting future risk from all climate-sensitive infectious diseases for the UK.
- The magnitude of this risk has not changed since CCRA3-IA-TR, even with the detection of new pathogens. This is because the new evidence has not been analysed thoroughly enough to understand changes in geographical patterns and future projections.
| Table 3.17: Urgency scores for H4 Risks to people from climate-sensitive infectious disease. Details of how the scores in this table were calculated are in the Methods Chapter. | |||||||
| ID | Risk | Present | 2030 | 2050 | 2080 | Urgency | |
| H4 | Risks to people from climate-sensitive infectious diseases | UK | M • • • | M • | M • | M • | MAN |
| England | M • • • | M • | M • | M • | MAN | ||
| Northern Ireland | M • • | M • | M • | M • | MAN | ||
| Scotland | M • • | M • | M • | M • | MAN | ||
| Wales | M • • | M • | M • | M • | MAN | ||
3.2.4.1 Evidence relevant to the entire United Kingdom
Current and future drivers of risk
The response of climate-sensitive infectious diseases to changes in weather and climate patterns depends on a complex mixture of human behaviour, host behaviour, human physiology, and pathogen sensitivity. Increased heatwaves and warmer annual temperatures can facilitate development, geographical spread, and active season of vectors like mosquitoes and ticks, raising the risk of diseases such as dengue and Lyme disease. They can also enhance bacterial proliferation, heightening incidences of food and water-borne illnesses. Hotter periods, including milder winters, can accelerate pathogen development rate and extend or lengthen the period of the year when infection risk is greatest. For instance, cases of food-borne disease infections such as Salmonella and Campylobacter are highest during the summer, but may become common in spring/autumn or even during warmer-than-average winter seasons (Kuhn et al., 2020). Sustained changes in climate patterns may allow for the establishment and survival of non-native vectors, as well as warm water-related pathogens such as Vibrio spp. and blue-green algae. Conversely, some areas may become too hot or dry and thus unsuitable for survival of these vectors and pathogens. Climate change may also alter human behaviour, which can increase exposure to pathogens and vectors (e.g., due to increased water storage and visitation to green and blue spaces during hotter weather). Regarding water storage, there is currently little evidence to distinguish the risks associated with public and private supplies, though a scoping review conducted by Public Health Wales (2023e) suggested private supplies may have a low(er) level of compliance to water quality standards.
Beyond temperature, other weather changes may also be important. For example, changing humidity may alter pathogen and vector survival rates and changing rainfall may affect transmission pathways. Extreme rainfall and river flooding during summer months in England has already resulted in extremely high densities of mosquitoes, causing nuisance biting to local residents (Vaux et al., 2021).
Certain vulnerable groups face heightened risks from climate-sensitive diseases, including older adults, young children, pregnant people, individuals with chronic health conditions, socio-economically disadvantaged populations, and communities with limited healthcare access (Paavola, 2017). Those who live or work rurally, as well as people taking part in certain types of work, sports and recreations may be at risk, including outdoor workers, hikers and recreational water users (such as wild swimmers or surfers). In addition, people living in flood-prone areas may be at risk from mosquitoes and waterborne pathogens following floods.
Risk interactions: Climate change will have effects on infectious diseases in many countries outside of the UK. International trade and travel are key pathways through which these global effects may impact the UK through the introduction of diseases and vectors into the UK (Reisen et al., 2009), especially if climate change creates local conditions which are suitable for the vector’s establishment. The development of adaptative measures such as urban greening and increasing biodiversity can offer opportunities for improved health and wellbeing. If these spaces are inadequately developed, however, they may inadvertently create favourable habitats for disease-transmitting mosquitoes and ticks, bringing people into closer contact with them (Smith et al., 2024).
Higher infection rates may increase health service demand (H6), leading to delays in care for other conditions and impacting overall health outcomes for the population. Treatment may require antibiotics, which may increase opportunities for anti-microbial resistance to arise. Changes to the geographical spread and prevalence of pathogens may impact food security (N11). Flooding and drought (H2) increase the risk of bathing and drinking water sources being contaminated with pathogens.
Assessment of current magnitude of risk
The incidence of many infectious diseases has changed over time, but it is unclear to what degree these changes can be attributed directly to climate change as food hygiene practices have improved (Lake et al., 2009), vaccination programmes have been introduced (for example, rotavirus (Atchison et al., 2016), and trade, travel and urbanization have impacted disease spread.
For some climate-sensitive infectious diseases (such as Salmonella, Campylobacter and Vibrio) there is good evidence of the climatic impact on an increase in case numbers and/or pathogen presence, even if absolute numbers are hard to establish. However, there are some pathogens where the relationship between weather variables and disease is lacking, particularly for different regions of the UK (see below sections). There is good evidence of the impact of weather on vectors and vector-borne diseases, although it is incredibly difficult to ascertain the impact of weather alone. For example, the impact on health from reduced recreational water quality is considered low, which is largely based on the lack of evidence for deaths in systematic or semi-systematic synthesis of both observational and non-observational studies.
As such, the current magnitude scores for all four nations have been assessed as medium, reflecting the current burden of climate sensitive diseases. The confidence around the magnitude score for most nations is medium, although Northern Ireland is scored a low due to the lack of studies based in Northern Ireland compared with the other nations.
Foodborne and waterborne infections
Campylobacter: Bacteria that cause diarrheal illness and is often associated with foodborne transmission (Fischer, Hashmi and Paterek, 2024), although wider environmental exposures may also be important. Many UK-based studies show Campylobacter incidence increases as temperatures increase, up to a threshold, but uncertainty remains in the literature as to the casual mechanism with some conflicting results (Louis et al., 2005; Tam et al., 2006; Lake et al., 2009; Sanderson et al., 2018; Djennad et al., 2019; Iacono et al., 2024).
Salmonella: Bacteria that cause food poisoning from contaminated meat, eggs, or water, and prevalence increases with temperature (Kovats et al., 2004; Lake et al., 2009). For example, in Scotland, there was a 4.7% increase in Salmonella cases for every degree rise over a 3°C threshold (95% CI: 2.1-7.3), whilst in England and Wales there was a 12.4% increase in Salmonella cases per every degree rise over a 5°C threshold (95% CI: 11.6-13.3) (Kovats et al., 2004). Similarly, there was a positive association with cases of the two most reported types of Salmonella (serovars) (Salmonella Enteritidis and Salmonella Typhimurium) and temperature (current and previous week) in England and Wales (Lake et al., 2009).
Vibrio: Bacteria that cause severe skin and gastrointestinal infections that thrive and multiply in warm waters and are naturally found in coastal waters (Vezzulli et al., 2016). Infection can occur following consumption of raw or undercooked seafood or fish, as well as ingestion or exposure to contaminated water. Increases in coastal water temperatures have resulted in the detection of some vibrio species in UK shellfish samples (Harrison et al., 2022). During the 2018 heatwave event and into 2019, Vibrio parahaemolyticus, Vibrio vulnificus and Vibrio cholerae were present at high concentrations in water samples from one UK estuarine site, with greater abundances corresponding to higher water temperatures and lower salinity (Ford et al., 2020).
Shiga toxin-producing Escherichia coli (STEC): A group of E. coli bacteria normally transmitted through contaminated food that produce harmful toxins, which cause severe infection in humans (ECDC, 2025). An outbreak in 2022 was likely caused by UK-grown lettuce crops becoming contaminated during an adverse flooding event, where following drought-like conditions, two months of rain fell in the region over a 24-hour period (Cunningham et al., 2024).
Cryptosporidium: A water-borne and food-borne parasite that causes cryptosporidiosis (UKHSA, 2024n). One study using data from the 1990s reported a 27% increase in cases if the cumulative rainfall in the preceding week was high (Naumova et al., 2005). However, in the early 2000s, drinking water regulations were strengthened and many recent outbreaks, such as the outbreak of >100 cases in Devon, are associated with faulty infrastructure (BBC News, 2024). However, such system vulnerabilities can be amplified by adverse weather events (further information in I9: risks to water supply and wastewater systems).
Norovirus: A virus, often spread through contaminated food, that causes vomiting and diarrhoea (NHS, 2024). For England and Wales, one study found a 15% reduction in norovirus reports if the month preceding was 1°C warmer, whereas a 1% increase in relative humidity led to a 2% decrease in reports (Lopman et al., 2009).
Rotavirus: A virus that primarily causes gastroenteritis, particularly severe diarrhoea, vomiting, fever, and abdominal pain in infants and young children (CDC, 2024). An inverse relationship with temperature has been reported (Atchison et al., 2009). The effect of temperature was broadly similar in England, Wales and Scotland, ranging from 7%-16% decrease in cases per 1°C rise in mean weekly temperature (Atchison et al., 2009).
Air-borne infections
Legionella: A bacterium that can cause respiratory illnesses in humans through inhalation of contaminated airborne water droplets (NHS, 2023), with increases in risk associated with increases in temperature in the preceding two months and increases in rainfall in the preceding week (Halsby et al., 2014).
Airborne viruses: For some pathogens, such as adenoviruses, respiratory syncytial virus (RSV), influenza A and B viruses and human metapneumovirus, temperatures were significantly colder on days when the pathogens were detected compared with days where they were not, and in some cases increased temperatures causes shortened infection seasons (Donaldson, 2006). In contrast, there were other pathogens such as rhinoviruses and human parainfluenza viruses where there was no significant difference in abundance between warmer and colder days (Price, Graham and Ramalingam, 2019). Seasonal coronavirus cases (not including SARS-COV-2) were significantly higher when air temperatures were below 10°C and relative humidity was above 84% in the two weeks preceding diagnosis (Nichols et al., 2021).
Vectors and vector-borne diseases
Ticks and associated diseases: In the UK, the sheep tick (Ixodes ricinus) is the most widely distributed tick species, and most likely to bite people and carries the bacteria which causes Lyme disease. It is found in a range of habitats including woodland, heathland, grazed and scrub grassland, urban parks and gardens. Passive surveillance conducted by the UK Health Security Agency (UKHSA) suggests tick distribution has expanded across much of the UK in recent years, which may be driven by several factors including changes in weather and climate, but also woodland cover and connectivity, deer densities and human behaviour (Gandy, Hansford and Medlock, 2023). The number of ticks infected with the Lyme disease bacteria is also different across habitats (Cull et al., 2021; Medlock et al., 2022). This highlights the importance of considering that biodiversity initiatives to increase woodland cover through planting trees, woodland regeneration and rewilding could alter the microclimate and increase habitat availability for ticks and hosts (UKHSA, 2024d (HECC chap.8)).
Since 2019, there have been several probable cases of tick-borne encephalitis virus (TBEv) acquired in the UK, as well as seropositivity (test results suggesting previous exposure to the virus) of deer detected (Kreusch et al., 2019; Mansbridge et al., 2022; Callaby et al., 2025). Deer were more likely to be positive for TBEv in sites with a high percentage cover of coniferous woodland, and higher rate of spring warming or mean annual surface temperature (Hassall et al., 2025).
As the UK experiences warmer temperatures and changing rainfall patterns due to climate change, conditions may become more conducive for mosquitoes to survive and breed. The mosquitoes of primary concern for disease transmission currently and in a changing climate include species belonging to the Anopheles, Aedes and Culex genera. Culex modestus, a vector for West Nile Virus, is being found in more locations around the UK, especially in the south, but also as far north as Suffolk (Vaux et al., 2024). West Nile Virus was detected in UK mosquitoes (Aedes vexans) for the first time in July 2023 (Bruce et al., 2025). Evidence from the USA, where the first detection of West Nile Virus was in New York in 1999, suggests it spreads geographically at a fast rate, and is extremely difficult to eradicate (Colpitts et al., 2012). Eggs of Aedes albopictus, a vector for several infections including dengue, were first detected in a motorway service station in Kent in September 2016 (Medlock et al., 2017), and there have been further detections of eggs and larvae since (Vaux et al., 2019; Johnston et al., 2025). Locally transmitted dengue outbreaks have now occurred in neighbouring countries, including in parts of northern France (Arulmukavarathan et al., 2024), emphasising the importance of preventing this species becoming established. Although Anopheles mosquitoes (the vectors of malaria) are present in the UK, and imported cases are routinely reported, there have been several cryptic malaria cases, where there is no recent travel history to a malaria-endemic country in the past few years (UKHSA, 2024l). However, due to an effective UK treatment and monitoring system, malaria is considered unlikely to re-establish.
Antimicrobial resistance
Antimicrobial resistance (AMR) refers to the capacity of microorganisms to withstand the effects of antimicrobial treatments, such as antibiotics. It is a leading cause of deaths, and it has been estimated that globally in 2021 there were 1.14 million deaths directly attributed to bacterial AMR and 4.71 million deaths associated with it (Naghavi et al., 2024). Changes in infectious diseases from weather and climate patterns interact with changes in antibiotic usage, and therefore potentially affect AMR. However, understanding of the impact that climate change is having on AMR is currently limited and requires further research (van Bavel et al., 2024).
Assessment of future magnitude of risk
There are only a small number of studies, predominately focusing on vectors and vector-borne diseases which have quantified future risk. If infections are not mentioned in the proceeding sections, then it is because there are currently no studies quantifying future risk. Unless stated otherwise, all studies have used a high emissions scenario (RCP8.5) and are described in the following section. Magnitude scores for low or central scenarios are often inferred from the high scenario, thereby decreasing our confidence in that evidence. Many of the pathogens mentioned in the previous sections have not been looked at under any climate scenario, so are omitted from the below.
Vibrio: As temperatures increase, UK coastal waters will become more favourable for the growth of Vibrio and the risk of outbreaks is likely to increase (Baker-Austin et al., 2017). Modelling studies using both medium (SSSP2-4.5) and high emission scenarios suggest that, in future, there will be an increase in UK coastline suitable for the growth and survival of Vibrio compared with current conditions (Trinanes and Martinez-Urtaza, 2021).
Aedes albopictus and associated diseases: Climate modelling suggests the London area is already suitable for A. albopictus, and it has been estimated using a high scenario that most of England will become suitable for established populations as early as the 2040s or 2050s, and most of Wales, Northern Ireland, and parts of the Scottish Lowlands becoming suitable as early as the 2060s or 2070s (UKHSA, 2024d (HECC chap.8)). Dengue could become endemic in London during the 2060s under a high scenario (Liu-Helmersson et al., 2016). Modelling suggests that during 2000-2022, temperatures were warm enough during some years for potential transmission of chikungunya to occur in London and parts of the East of England (UKHSA, 2024d (HECC chap.8)). In the future, as temperatures continue to increase, modelling using a high scenario suggests more areas across the UK are predicted to exceed required threshold temperatures, with many parts of England and Wales predicted to be warm enough for potential transmission during three consecutive months and reaching four months in London by the 2070s (UKHSA, 2024d (HECC chap.8)). There may also be increased risk from diseases such as dengue for UK residents travelling overseas, as modelling has estimated an increase in dengue incidence of 49%-76% in Asia and the Americas depending on the emissions scenario (Childs et al., 2025).
Hyalomma marginatum: Climate projection data using a high scenario suggests that whilst UK temperatures will increase in future, autumn temperatures on average are likely to remain too cold for nymphs to moult to adults and affect survival over the winter, although there were variations between different model runs (UKHSA, 2024c (HECC chap.7)).
West Nile virus: Modelling studies of future risks using a high scenario show most of southern England and parts of the Midlands are predicted to be at risk of West Nile virus outbreaks by mid-century (Ewing et al., 2021; Withers et al., 2024). The risk of infection with West Nile virus is currently low but is predicted to increase into the second half of this century throughout lowland England and parts of Wales (Ewing et al., 2021).
Level of preparedness for risk
The UK Biological Security Strategy (Cabinet Office, 2025b) provides the framework to make the UK resilient to biological threats. Its mission is to understand current and future biological risks, prevent risks from emerging where possible, and to detect and respond to risks to lessen the impact on the UK.
UK policy on managing emerging infections is addressed through the multi-agency cross-government horizon scanning and risk assessment Human Animal Infections Risk Surveillance (HAIRS) group (UKHSA, 2025e). The UK government launched the Third National Adaptation Programme (NAP3) in 2023 (Defra, 2024c), which includes enhancing surveillance, undertaking horizon scanning and conducting research to monitor changes in vector-borne disease distribution in the UK and worldwide. Within the NAP, UKHSA has a remit to update the evidence base for the impacts of climate change on health in the UK, which includes infectious diseases.
The Food Standards Agency (FSA) is responsible for food safety and food hygiene in England, Wales, and Northern Ireland and Food Standards Scotland is responsible for food safety and food hygiene in Scotland. The FSA’s Food System Strategic Assessment 2023 (Food Standards Agency, 2023) recognised that foodborne and zoonotic diseases may increase in the UK over the next decade. It suggested actions to achieve more comprehensive and regular global monitoring and data sharing, as well as stronger food safety enforcements along supply chains. FSA are developing a new Area of Research Interest (ARI) to focus on understanding the potential impacts on the UK of changing food availability, food security and food safety risks (Food Standards Agency, 2024).
Assessment of the evidence base and evidence gaps
There is currently a lack of studies attributing the burden of infectious diseases to specific weather and climate factors in the UK. There needs to be more studies that project future infectious disease risk, including emergence of novel infections, using a combination of different warming and adaptation scenarios. There is also a relative lack of studies across these diseases in individual countries of the UK, especially Northern Ireland.
3.2.4.2 England
Additional evidence provided here is specific to England. Where diseases are not mentioned, no additional information was available and evidence for the UK (3.2.4.1) was used to assess risk.
Assessment of current magnitude of risk
For the risk posed by recreational seawater, a crude estimate can be made from the only randomised controlled trial conducted in the UK (England and Wales) between 1989-1992. The results of this trial indicated that the largest differences in seawater quality – defined as seawater with 0-13 ml faecal streptococci (an indicator of sewage pollution) versus 50-158 ml faecal streptococci – are associated with approximately 15,000 more gastrointestinal infections per 100,000 outdoor seawater users every year (Fleisher et al., 1993, 1996, 1998; Kay et al., 1994; Fleisher and Kay, 2006). Therefore, the magnitude of current effects on recreational water users would be expected to fall in the low-to-medium range. However, it is difficult to be more specific and disentangle the current effects of weather and climate change, versus existing waste management processes and infrastructure in the UK (e.g., combined sewerage, regulation of water industry). Higher sea-surface temperatures and lower salinity have also resulted in the detection of more novel human pathogenic Vibrio species in shellfish sampled from English coastline sites (Ford et al., 2020; Harrison et al., 2022). An equivalent UK randomised trial does not exist for freshwater and Vibrio risk does not apply to freshwaters, though the results of a trial conducted in Germany suggest risks attributable to reduced freshwater quality are similarly in the order of thousands per 100,000 (Wiedenmann et al. 2006).
There has been a reduction in rotavirus reports in England, Wales and Scotland with increasing mean temperature (Atchison et al., 2009). Lastly, there is evidence of an increase in cryptosporidiosis rate by 27% in northern England if cumulative rainfall for prior week was in 75th percentile (Naumova et al., 2005).
Higher seasonal coronavirus cases are observed during low temperature, high humidity periods in England (Nichols et al., 2021). Higher temperatures due to climate change may reduce the risk of norovirus transmission as a 15% reduction in norovirus reports followed where the month preceding was 1°C warmer, whereas a 1% increase in relative humidity led to a 2% decrease in reports in England and Wales (Lopman et al., 2009). Similarly, lower rotavirus cases have been reported at higher temperatures in England after controlling for trend, seasonality, public holidays, relative humidity and rainfall (Atchison et al., 2009). Data from England and Wales suggests that the RSV season ended at a rate of 3.1 weeks earlier per 1 °C temperature rise, suggesting warmer temperatures shorten the season (Donaldson, 2006).
Ixodes ricinus is located across much of England (Hansford et al., 2026), and ticks infected with Lyme disease-causing bacteria have been detected in a number of different habitats (Cull et al., 2021; Medlock et al., 2022). There have been probable cases of TBE acquired in England, as well as seropositive (suggesting previous exposure to the virus) deer detected (Kreusch et al., 2019; Mansbridge et al., 2022; Callaby et al., 2025). Hyalomma marginatum is a non-native tick species found in southern Europe that carries Crimean-Congo haemorrhagic fever virus (CCHFV) (Walker, 2003; Choubdar et al., 2019). Migratory birds are important hosts of immature stages and can transport individual ticks over several thousand miles during spring migration. There have been several detections of this tick in England, including the most recent detection of a person with no history of travel (McGinley et al., 2021). It was hypothesised this was due to high temperatures facilitating the migration of birds as hosts (McGinley et al., 2021).
Culex modestus has spread from North Kent saltmarshes and Essex coast, to along the Thames Estuary in Kent, on the opposite bank in Essex and in the coastal wetlands of Essex. Eggs of Aedes albopictus, a vector for several infections including dengue, were first detected in a motorway service station in Kent in September 2016 (Medlock et al., 2017), and further detections of eggs and larvae have occurred in England since (Vaux et al., 2019; Johnston et al., 2025).
Assessment of future magnitude of risk
In the 2030s, a low emissions scenario (RCP2.6) leads to a 6.2% increase for non-tuberculous mycobacteria infections across the UK, and a 33.8% increase in infection rates to 10.2 cases per 100,000 people from 2023 to 2033 (Campbell et al., 2024). Secondly, an increase in UK coastline suitable for Vibrio is predicted (Trinanes and Martinez-Urtaza, 2021). For vector-borne diseases, modelling using high emissions scenarios (RCP8.5) suggests most of England and parts of Wales could become suitable for established populations of Aedes albopictus by the 2050s (UKHSA, 2024d (HECC chap.8)). High warming scenarios suggest that temperatures may be warm enough for potential chikungunya transmission during 1-2 consecutive months (UKHSA, 2024d (HECC chap.8)).
In the 2050s and 2080s, there is currently a scarcity of evidence showing the impact of low and central warming scenarios on climate-sensitive infectious diseases in England.
By 2080, high warming scenarios suggest England could become suitable for Aedes albopictus (UKHSA, 2024d (HECC chap.8)), with one study estimating dengue could become endemic in London during the 2060s (Liu-Helmersson et al., 2016). Many parts of England and Wales are predicted to be warm enough for potential chikungunya transmission for 3-4 consecutive months by 2080 (UKHSA, 2024d (HECC chap.8)). However, high warming scenarios suggest the threshold for self-sustaining populations of the tick species Hyalomma marginatum will not be met (Gillingham et al., 2023).
Level of preparedness for risk
The UKHSA’s mission is to prepare for, prevent and respond to health threats, save lives and protect livelihoods (UKHSA, 2023). There are specific priorities of UKHSA which all contribute to preparedness in the threat of climate change: to be ready to respond to all hazards to health; reduce the impact of infectious diseases and antimicrobial resistance; protect health from threats in the environment; and improve action on health security through data and insights. The impact of infectious diseases is also included within the National Risk Register (Cabinet Office, 2025a).
UKHSA regularly monitors infectious diseases in England (UKHSA, 2025e) and beyond through horizon scanning. The UKHSA preparedness plan (UKHSA, 2025f) highlights incident response plans, including levels for escalation/de-escalation, which is relevant to infectious disease outbreaks. The ‘Communicable disease outbreak management guidance’ (UKHSA, 2025b) provides health protection organisations in England with principles to support local health protection responses to communicable disease outbreaks, with the aim of preventing harm from such outbreaks. In 2025, the ‘Priority pathogen families reference tool’ (UKHSA, 2025g) was published, highlighting 24 pathogen families where further research is most needed in the interests of biosecurity. The tool also included a measure of climate sensitivity of pathogens, with many highlighting additional research is required. UKHSA has also published guidance on disease outbreak management to support local health protection systems (UKHSA, 2025b).
Invasive mosquito surveillance at ports was instigated in 2010 and has expanded to over 100 trapping localities at seaports, airports and highway transport hubs across England, Wales and Northern Ireland together with local health authorities and port health authorities. The National Contingency Plan for Invasive Mosquitoes is a cross-government document which outlines local-level actions to be taken in the event of a non-native mosquito detection (UKHSA et al., 2020). UKHSA also runs a Tick Surveillance Scheme (TSS) and has developed a tick awareness toolkit (UKHSA, 2024m), as well as resources for local authorities to raise awareness of ticks and tick-borne diseases in England. UKHSA works to provide evidence-based guidelines on adaptation for vectors and VBDs in England (Hawkes et al., 2020). One of UKHSA’s strategic priorities for 2023-2026 is to ‘reduce the impact of infectious diseases and antimicrobial resistance’ (UKHSA, 2023). UKHSA works with local authorities, who in turn may support community-led or citizen science approaches, to improve awareness and reduce the risk to health from VBDs. Surveillance and research partnerships are in place with UK academic institutions. Proactive habitat management also occurs through a range of organisations and partnerships.
In September 2024, the ‘Water (Special Measures) Bill’ was announced to target water company-related pollution of outdoor bathing waters in England and Wales. Amongst other measures, this bill increases the ability of the Environment Agency to fine and criminally charge law breaking (Defra, 2025c). The Environment Agency measure water quality regularly and advise on outdoor swimming in key locations in England.
Evaluation of urgency score
The overall risk in England is assessed as Medium for the current climate and future periods. This is based on the number of people exposed to harmful vector-borne, water-borne, and food-borne diseases, rather than air-borne diseases, which is likely to result in tens of deaths, hundreds of major health impacts and tens of thousands of people affected. This estimate is made from correlations of cases with temperatures, but no studies show actual population exposure to these diseases, so our confidence in the magnitude scores is Low. There is some modelling evidence around future vector-borne disease risk, but the evidence for other infections is much weaker. Confidence is Low for future risks, due to limited evidence of explicit climate drivers and a lack of England-specific projections. There is limited evidence of effective implementation and potential for other adaptation measures to inadvertently worsen the risk. These scores do not include the impact of climate change on AMR, which although is listed as an international element above also affects UK populations.
Table 3.18: Urgency scores for H4 Risks to people from climate-sensitive infectious diseases for England. Details of how the scores in this table were calculated are in the Methods Chapter.
| England | |||||||||
| H4 | Risks to people from climate-sensitive infectious diseases. | ||||||||
| Present | 2030 | 2050 | 2080 | ||||||
| Central | High | Central | High | Low | Central | High | |||
| No adaptation | M • • • | M • | M • | M • | M • | M • | M • | M • | |
| With adaptation | M • | M • | M • | M • | M • | M • | M • | ||
| Urgency scores | MAN | FI | FI | FI | |||||
| Overall urgency score | MAN | ||||||||
3.2.4.3 Northern Ireland
Additional evidence here is specific to Northern Ireland. Where diseases are not mentioned, no additional information was available and evidence for the UK (3.2.4.1) was used to assess risk.
Assessment of current magnitude of risk
There is currently a lack of evidence relating specifically to climate-sensitive diseases in Northern Ireland. However, it is likely that correlations between disease cases and weather seen in other UK nations will also apply in Northern Ireland, although temperature thresholds for diseases/vectors may be different.
Assessment of future magnitude of risk
A low warming scenario is predicted to result in a 7.5% increase in non-tuberculous mycobacteria infection rates in Northern Ireland by 2033 (Campbell et al., 2024). In addition, the coastline around Northern Ireland which is suitable for Vibrio is predicted to increase by 2100 (Trinanes and Martinez-Urtaza, 2021).
For vector-borne diseases, modelling using high warming scenarios suggests parts of Northern Ireland could become suitable for the establishment of Aedes albopictus by the 2060s or 2070s (UKHSA, 2024d (HECC chap.8)). High warming scenarios suggest temperatures are unlikely to be warm enough for potential chikungunya transmission, even by 2080 (UKHSA, 2024d (HECC chap.8)).
Level of preparedness for risk
The Health Protection Service within the Northern Ireland Public Health Agency (PHA) has the lead role in protecting the population from infection and undertakes surveillance and monitoring of pathogens. The second Northern Ireland Climate Change Adaptation Programme (NICCAP2) (DAERA, 2019) reports on actions to address disease risks for plants and wildlife, but no actions are listed for human pathogens.
The NICCAP2 (DAERA, 2019) highlights that some evidence has pointed to recent declines in bathing water quality in Northern Ireland and mentions the ‘System for Bathing Water Quality Monitoring’ (SWIM) that will investigate and model the linkage between heavy rainfall events and poor bathing water quality. It also refers to ‘Sustainable Water – A Long-Term Water Strategy for Northern Ireland (2015–2040)’, which recognises that all policies must factor in the future implications of climate change on both quality and quantity of water resources. It also notes that the ‘Drinking Water and Health Guidance’ is reviewed annually and contains action to be taken should drinking water quality fall below health-based criteria. Northern Ireland’s ten year ‘Making Life Better’ strategy for health and wellbeing has an objective to provide safe and clean drinking water. The SWIM project is now complete for six sites, and water quality predictions are delivered during the bathing season on the ‘SWIM NI’ app.
Each year, UKHSA conducts invasive mosquito surveillance at over 100 trapping localities at seaports, airports and highway transport hubs with local health authorities and port health authorities across England, Wales and Northern Ireland.
Evaluation of urgency score
The overall risk in Northern Ireland is assessed as Medium for the current climate and future periods. This is based on the number of people exposed to harmful vector-borne, water-borne, and food-borne diseases, rather than air-borne diseases, which is likely to result in tens of deaths, hundreds of major health impacts and tens of thousands of people affected. There is some modelling evidence around future vector-borne disease risk, but the evidence for other infections is much weaker. Confidence is Low for future risks due to limited evidence of explicit climate drivers and a lack of Northern Ireland-specific projections. There is limited evidence of effective implementation and potential for other adaptation measures to inadvertently worsen the risk. These scores do not include the impact of climate change on AMR which, although listed as an international element above, also affects UK populations.
Table 3.19: Urgency scores for H4 Risks to people from climate-sensitive infectious diseases for Northern Ireland. Details of how the scores in this table were calculated are in the Methods Chapter.
| Northern Ireland | |||||||||
| H4 | Risks to people from climate-sensitive infectious diseases. | ||||||||
| Present | 2030 | 2050 | 2080 | ||||||
| Central | High | Central | High | Low | Central | High | |||
| No adaptation | M • • | M • | M • | M • | M • | M • | M • | M • | |
| With adaptation | M • | M • | M • | M • | M • | M • | M • | ||
| Urgency scores | MAN | FI | FI | FI | |||||
| Overall urgency score | MAN | ||||||||
3.2.4.4 Scotland
Additional evidence here is specific to Scotland. Where diseases are not mentioned, no additional information was available and evidence for the UK (3.2.4.1) was used to assess risk.
Assessment of current magnitude of risk
A mean temperature increase of 1 °C reduces the odds of detecting adenovirus (2.8%), RSV (17.3%), influenza A (13.7%) and influenza B (13%) viruses and human metapneumovirus (9.9%) in Scotland (Price et al., 2019). Cases of some respiratory diseases are also linked with relative humidity, including human metapneumovirus, RSV, influenza A virus in Scotland (Price et al., 2019). Higher rotavirus cases have been reported at lower temperatures in Scotland after controlling for trends, seasonality, public holidays, relative humidity and rainfall (Atchison et al., 2009).
Assessment of future magnitude of risk
A low warming scenario is predicted to result in a 9.5% increase in non-tuberculous mycobacteria infection rates in Scotland by 2033 (Campbell et al., 2024). In addition, the length of coastline around Scotland which is suitable for Vibrio is predicted to increase by 2100 (Trinanes and Martinez-Urtaza, 2021).
For vector-borne diseases, modelling using high warming scenarios suggests parts of the Scottish Lowlands could become suitable for the establishment of Aedes albopictus by the 2060s or 2070s (UKHSA, 2024d (HECC chap.8)). High warming scenarios suggest temperatures are unlikely to be warm enough for potential chikungunya transmission in Scotland, even by 2080 (UKHSA, 2024d (HECC chap.8)).
Level of preparedness for risk
Preparedness and adaptation efforts have a particular focus on Lyme disease due to its increasing public health relevance in Scotland. The Scottish Government published the Scottish National Adaptation Plan 2024 – 2029 (Scottish Government, 2024c), known as SNAP 3, and an associated monitoring and evaluation framework (Scottish Government, 2025b). SNAP 3 recognises that climate change is already affecting VBD transmission and spread, and that policy responses to climate change, including ecosystem services, could create habitats more suitable for vectors. The Scottish Government have led a multi-media communications campaign, ‘Find a tick remove it quick’, over consecutive summers (2023/2024), which have helped raise the profile of VBD threats in Scotland. SNAP 3 has committed over the five-year plan to mapping the risk of emergent VBD due to climate change, scoping enhanced surveillance, scoping adoption of VBD contingency plans for England and horizon scanning for VBD of livestock. The Scottish Government continues to work with partners to progress these commitments. Health Protection Scotland published updated information on ticks and Lyme disease in Scotland in 2018, including guidance on prevention and treatment. The National Surveillance of Gastrointestinal Infections and Zoonoses in Scotland report provides information on reported laboratory-confirmed cases of pathogens in Scotland during 2015-2024 (Public Health Scotland, 2025a).
SEPA monitors and publishes the general microbiological quality of the water at outdoor swimming sites during bathing season. PHS manage the Scottish Environmental Incident Surveillance System (SEISS), a database holding details of incidents where there may be a risk to public health due to the release into the environment of chemical, microbiological, radiation or other physical agents.
Evaluation of urgency score
Across climate sensitive diseases assessed, the magnitude scores are the same as other UK nations. The overall risk in Scotland is assessed as Medium for the current and future periods. This is based on an estimate of the number of people exposed to harmful vector-borne, water-borne, and food-borne diseases, which is likely to result in tens of deaths, hundreds of major health impacts and tens of thousands of people affected. This estimate is made from correlations of cases with temperatures, but no studies show actual population exposure to these diseases, so our confidence in the magnitude scores is Low. There is some modelling evidence around future vector-borne disease risk, but the evidence for other infections is much weaker. Confidence is Low for future risks, due to limited evidence of explicit climate drivers and a lack of Scotland-specific projections. There is limited evidence of effective implementation and potential for other adaptation measures to inadvertently worsen the risk. These scores do not include the impact of climate change on AMR which, although listed as an international element above, also affects UK populations.
Table 3.20: Urgency scores for H4 Risks to people from climate-sensitive infectious diseases for Scotland. Details of how the scores in this table were calculated are in the Methods Chapter.
| Scotland | |||||||||
| H4 | Risks to people from climate-sensitive infectious diseases. | ||||||||
| Present | 2030 | 2050 | 2080 | ||||||
| Central | High | Central | High | Low | Central | High | |||
| No adaptation | M • • | M • | M • | M • | M • | M • | M • | M • | |
| With adaptation | M • | M • | M • | M • | M • | M • | M • | ||
| Urgency scores | MAN | FI | FI | FI | |||||
| Overall urgency score | MAN | ||||||||
3.2.4.5 Wales
Additional evidence here is specific to Wales. Where diseases are not mentioned, no additional information was available and evidence for the UK (3.2.4.1) was used to assess risk.
Assessment of current magnitude of risk
Higher seasonal coronavirus cases are observed during low temperature, high humidity periods in Wales (Nichols et al., 2021). There is a 15% reduction in norovirus reports if the month preceding was 1 °C warmer, whereas a 1% increase in relative humidity led to a 2% decrease in reports in England and Wales (Lopman et al., 2009, p. 200). Similarly, higher rotavirus cases have been reported at lower temperatures in Wales after controlling for trend, seasonality, public holidays, relative humidity and rainfall (Atchison et al., 2009). Data from England and Wales suggests that the RSV season ended at a rate of 3.1 weeks earlier per 1 °C temperature rise, suggesting that warmer temperatures shorten the season (Donaldson, 2006). For recreational (sea)water quality risks, the discussion for England above is also relevant here since the randomised trial mentioned was also conducted in Wales and the two regions are climatologically similar and hence may respond similarly to emerging Vibrio pathogens too.
Assessment of future magnitude of risk
A low warming scenario is predicted to result in a 0.9% increase in non-tuberculous mycobacteria infection rates in Wales by 2033 (Campbell et al., 2024). In addition, the coastline around Wales suitable for Vibrio is predicted to increase by 2100 (Trinanes and Martinez-Urtaza, 2021).
For vector-borne diseases, modelling using high warming scenarios suggests most of Wales could become suitable for the establishment of Aedes albopictus by the 2060s or 2070s (UKHSA, 2024d (HECC chap.8)). High warming scenarios suggest temperatures in parts of South Wales could be warm enough for potential chikungunya transmission for 1-3 consecutive months by 2080 (UKHSA, 2024d (HECC chap.8)). However, high warming scenarios suggest the threshold for self-sustaining populations of the tick species Hyalomma marginatum will not be met (Gillingham et al., 2023).
Level of preparedness for risk
The Climate Adaptation Strategy for Wales (Welsh Government, 2024b) mentions a ‘One Health’ approach to minimise the threat of transmission of domestic animal diseases to wildlife and vice versa. This includes collaborating on the surveillance of vectors and diseases, real-time assessment of threats from diseases in other countries, and developing preparedness and response capability for exotic diseases, including horizon-scanning for emerging threats overseas. In addition, Public Health Wales (PHW) are incorporating climate indicators into routine gastrointestinal surveillance reports and have produced a Wales-specific non-foodborne zoonoses report focusing on climate-sensitive pathogens (not publicly available). A health and social care climate adaptation toolkit (Welsh Government, 2024d) has been produced, which includes climate-sensitive diseases as a risk that needs to be understood and considered during planning.
The climate related risk from vector-borne pathogens is recognised in the Welsh Government’s adaptation plan, Prosperity for All: A Climate Conscious Wales (Welsh Government, 2019). One particular action seeks to increase understanding of the risk, with continued monitoring at ports and airports, and efforts to increase understanding of the risk, particularly from Lyme disease, with healthcare professionals. The plan commits to research what other action is needed and to survey where vectors are entering Wales in the future. There is a recognition that increased use of blue / green infrastructure as ecosystem services to other climate threats could increase the problem with native vectors, and therefore there is a commitment to work on avoiding this issue, working with Natural Resources Wales and other experts. This will include putting in place effective measures for urban and peri-urban blue and green space to prevent habitats for vectors. PHW are also collaborating with UKHSA and working closely with local authorities to extend mosquito surveillance in Wales. Each year, UKHSA conducts invasive mosquito surveillance at over 100 trapping localities at seaports, airports and highway transport hubs with local health authorities and port health authorities across England, Wales and Northern Ireland.
Prosperity for All: A Climate Conscious Wales also highlighted the Welsh Government’s Water Strategy for Wales (2015a), which aims to maintain high levels of water quality and protect the health of people in Wales. The strategy identifies the risks from climate change and is underpinned by an all-Wales action plan. In addition, the Water Health Partnership for Wales is an initiative that brings together relevant agencies to work together more effectively to protect public health by ensuring the provision of safe drinking water. Agencies in the Partnership include the Drinking Water Inspectorate, Welsh Government, local authority public and environmental health, water companies and Public Health Wales. Natural Resources Wales is the regulatory body responsible for managing water resources in Wales. They provide oversight of both Bathing and Drinking Water in Wales through a wide range of strategies and plans and regulatory activity. Water companies also report annually on bathing water quality in Wales (Natural Resources Wales, 2025).
PHW’s Climate Change Programme Board (CCPB) has established the Climate Change Surveillance Sub-Group, consisting of internal and external partners, including the Welsh Government and the Office for National Statistics. The CCPB’s programme strategic decisions are informed by and shared with the Welsh Government Adaptation National Project Board and Health Protection Advisory Group Environmental Public Health Subgroup. The PHW Climate Change Surveillance Sub-Group will initially focus on the development of heat morbidity and mortality surveillance.
Evaluation of urgency score
The overall risk in Wales is assessed as Medium for current and future periods. This is based on the number of people exposed to harmful vector-borne, water-borne, and food-borne diseases, rather than air-borne diseases, which is likely to result in tens of deaths, hundreds of major health impacts and tens of thousands of people affected. There is some modelling evidence around future vector-borne disease risk, but the evidence for other infections is much weaker. Confidence is Low for future risks due to limited evidence of explicit climate drivers and a lack of Wales-specific projections. There is limited evidence of effective implementation and potential for other adaptation measures to inadvertently worsen the risk. These scores do not include the impact of climate change on AMR which, although listed as an international element above, also affects UK populations.
Table 3.21: Urgency scores for H4 Risks to people from climate-sensitive infectious diseases for Wales. Details of how the scores in this table were calculated are in the Methods Chapter.
| Wales | |||||||||
| H4 | Risks to people from climate-sensitive infectious diseases. | ||||||||
| Present | 2030 | 2050 | 2080 | ||||||
| Central | High | Central | High | Low | Central | High | |||
| No adaptation | M • • | M • | M • | M • | M • | M • | M • | M • | |
| With adaptation | M • | M • | M • | M • | M • | M • | M • | ||
| Urgency scores | MAN | FI | FI | FI | |||||
| Overall urgency score | MAN | ||||||||
3.2.5 Risks to food safety and nutrition – H5
Risk to food safety and nutrition is inherently linked to food security, which is covered in the Land, Nature, and Food chapter (risk N11). An important component of food safety is infection caused by specific food-borne pathogens, some of which are climate sensitive. These are discussed and included in magnitude scores in the infectious diseases risk (H4) (see also Box 3.7 below). CCRA3-IA TR expands on CCRA3-IA TR by considering nutrition alongside food safety, and in addition to food security. This recognises the importance of both food and nutrition security (quantity and quality of food), and the health and social value of food above and beyond the provision of sufficient calories or food as a tradeable commodity. Evidence on the impact of climate change on nutrition and diet-related health outcomes in the UK, however, is scarce.
Headlines
- Further investigation is needed to assess urgency due to limited evidence directly linking climate change to UK food safety and diet-related morbidity and mortality.
- Inequality in accessing safe and nutritious food is likely, especially for fresh fruits and vegetables. This is due to a reliance on imported food and increased global climate-related food production shocks and food trade/price volatility.
- Devolved administrations have adaptation plans in place or in development. How these will be implemented or impact food safety and nutrition security is uncertain.
- The urgency score (Further investigation) remains unchanged from CCRA3-IA-TR, despite the remit of this risk no longer including food security.
| Table 3.22: Urgency scores for H5 Risks to food safety and nutrition. Details of how the scores in this table were calculated are in the Methods Chapter. | |||||||
| ID | Risk | Present | 2030 | 2050 | 2080 | Urgency | |
| H5 | Risks to food safety and nutrition | UK | M • | M • | M • | M • | FI |
| England | M • | M • | M • | M • | FI | ||
| Northern Ireland | M • | M • | M • | M • | FI | ||
| Scotland | M • | M • | M • | M • | FI | ||
| Wales | M • | M • | M • | M • | FI | ||
3.2.5.1 Evidence relevant to the entire United Kingdom
Current and future drivers of risk
The impact of changes in climate or climate induced extreme weather events on UK food safety, diets, and nutrition can be complex, with limited evidence available to quantify or qualify direct or compounding and cascading risks. Extreme weather events and other changes related to climate change may impact the quantity, quality, diversity, and accessibility of foods in the UK via different pathways throughout global and domestic food systems. These effects may in turn increase the risk of consuming foods that are unsafe and can make it more challenging to consume diets which meet national nutritional guidelines.
Hotter environments increase the likelihood of food spoilage and proliferation of pathogens (Damtew et al., 2024). High humidity, especially in warmer seasons, can worsen the risk of fungal growth, such as moulds, and lead to spoilage of non-refrigerated stored food products. Waterlogging is linked to crop losses and reduced quality of crops in terms of nutrition and toxicology. Rising atmospheric CO₂ concentrations may increase yields but also reduce the nutritional quality of certain crops. Flooding, storms, and sea water intrusion can contaminate crops, food, and water sources, disrupt food storage and cold chain systems, and increase the proliferation of specific food-borne pathogens (see also H4, 3.2.4). Disruption of infrastructure necessary for food handling and storage, such as cold chain systems, can exacerbate these risks. Changes to hygiene practices or pest and disease distributions across food systems because of climate change can pose a risk to food safety for UK populations if sufficient controls are not in place (UKHSA, 2024h (HECC chap.9)). Figure 3.3 shows how climate change can affect food safety and nutrition through multiple pathways.

Figure 3.3: The potential interactions of rising CO2 and climate change on food safety and nutrition from ‘farm to table’. (Taken from Maggiore et al., 2020).
Assessment of current magnitude of risk
The current magnitude of the risk is Medium across the UK. This is based on limited evidence that current climate conditions may impair the nutritional quality of key foods or the overall intake of diverse and nutrient dense foods, or may increase the risk of food safety incidents. All of these could in turn increase rates of illness for large numbers of people. Regarding the nutritional quality of foods, although rising levels of CO₂ increases some crop yields, they have a detrimental effect on the nutritional density of some plants and their harvestable parts (Ebi et al., 2018; Hoegh-Guldberg et al., 2019; Mbow et al., 2019). For example, rising CO₂ levels have been associated with reduced concentrations of nutrients in staple cereal crops (micronutrient or protein concentrations in wheat) (Myers et al., 2014; Ekele et al., 2025). These foods make a large contribution to intakes, so any reduction in nutrient density could have a major impact, especially in households with limited dietary diversity who are at risk of food insecurity or who are experiencing a high burden of diet-related poor health outcomes.
There is very little research directly attributing diet-related health outcomes to climate change or extreme weather events. Of the evidence available, the majority is related to undernutrition (undernourishment/ hunger, stunting, wasting) in climate vulnerable regions such as Sub-Saharan Africa, with some work focussing on dietary diversity, micronutrient deficiency, overweight/obesity, or considering diet-related non-communicable diseases, such as diabetes and heart disease (Salm et al., 2021; Fanzo et al., 2025). None of these studies specify the risk to UK populations at present, however they identify pathways to ill-health that may become relevant to the UK. For example, a study in the Pacific Islands linked climate change with trends in being overweight due to reduced availability of fruits and vegetables and over reliance on imported and processed food, showing how climate change effects can change food environments and health outcomes (McIver et al., 2016).
The UK population consistently misses targets for recommended fruits, vegetables, and fibre intake, with only one in ten adults consuming five fruits and vegetables a day. On average, the UK population derives approximately 40% of energy intake from Ultra Processed Foods (Chang et al., 2024; OHID, 2025). Maintaining the accessibility and affordability of good quality food, including fresh fruits and vegetables, and minimising any requirements to substitute these with Ultra Processed Foods is, therefore, a key priority to protect populations against diet-related disease (diet-related non-communicable diseases or micronutrient deficiency diseases).
Box 3.7 Food Poisoning
Some pathogens (bacteria, viruses and parasites), which cause infection or irritation of the digestive system when consumed in contaminated food are known to be sensitive to changes in climate (also see H4). While the health impacts of these food-borne pathogens are outlined here, they are not used to inform the overall urgency scoring for this risk.
Campylobacter: Bacteria that cause diarrheal illness and is often associated with foodborne transmission (Fischer et al., 2024), although wider environmental exposures may also be important. Many UK-based studies show Campylobacter incidence increases as temperatures increase, up to a threshold, but uncertainty remains in the literature as to the casual mechanism with some conflicting results (Louis et al., 2005; Tam et al., 2006; Lake et al., 2009, 2019; Sanderson et al., 2018; Djennad et al., 2019; Iacono et al., 2024).
Salmonella: Bacteria that cause food poisoning from contaminated meat, eggs, or water, and prevalence increases with temperature (Kovats et al., 2004; Lake et al., 2009). For example, in Scotland, there was a 4.7% increase in Salmonella cases for every degree rise over a 3°C threshold (95% CI: 2.1-7.3), whilst in England and Wales there was a 12.4% increase in Salmonella cases per every degree rise over a 5 °C threshold (95% CI: 11.6-13.3) (Kovats et al., 2004). Similarly, there was a positive association with cases of the two most reported types of Salmonella (serovars) (Salmonella Enteritidis and Salmonella Typhimurium) and temperature (current and previous week) in England and Wales (Lake et al., 2009).
Vibrio: Bacteria causing severe skin and gastrointestinal infections which naturally found in coastal waters and thrive and multiply in warm waters (Vezzulli et al., 2016). Infection can occur following consumption of raw or undercooked seafood or fish, as well as ingestion or exposure to contaminated water. Increases in coastal water temperatures have resulted in the detection of some vibrio species in UK shellfish samples (Harrison et al., 2022). During the 2018 heatwave event and into 2019, Vibrio parahaemolyticus, Vibrio vulnificus and Vibrio cholerae were present at high concentrations in water samples from one UK estuarine site, with greater abundances corresponding to higher water temperatures and lower salinity (Ford et al., 2020).
Shiga toxin-producing Escherichia coli (STEC): A group of E. coli bacteria normally transmitted through contaminated food that produce harmful toxins which cause severe infection in humans (ECDC, 2025). An outbreak in 2022 was likely caused by UK-grown lettuce crops becoming contaminated during an adverse flooding event, where following drought-like conditions, two months of rain fell in the region over a 24-hour period (Cunningham et al., 2024).
Norovirus: A virus, often spread through contaminated food, that causes vomiting and diarrhoea (NHS, 2024). For England and Wales, one study found a 15% reduction in norovirus reports if the month preceding was 1 °C warmer, whereas a 1% increase in relative humidity led to a 2% decrease in reports (Lopman et al., 2009).
Assessment of future magnitude of risk
Based on limited evidence the future risk is assessed as Medium across 2030s, 2050s and 2080s for all areas of the UK. The Food Standards Agency (2024) published a report on climate impacts on UK food systems and determined that in the near-term future (e.g., next five years), environmentally driven changes will result in increased volatility for supply chains; increased risks to the accessibility of diverse and nutritious foods exacerbating inequalities in food insecurity; and increased food safety risks across supply chains. These effects will make it more difficult to increase the proportion of the UK population who meet government dietary recommendations (especially in lower income and underserved or vulnerable households).
Level of preparedness for risk
All four of the UK nations have a cross-departmental food strategy, with England being the latest to release their report in 2025 (Defra, 2025a). Responsibility for adaptation lies with government bodies, public health agencies, and key sectors including agriculture, health, and food safety authorities, each working to address specific regional challenges while aligning with national strategies. The monitoring and surveillance of food safety and nutrient security is part of an obligation for Defra to report on food security every year (UK Agriculture Act 2020). Diets are also monitored across the UK through a variety of national surveys, some of which are conducted on a rolling basis (e.g., The National Diet and Nutrition Survey, NDNS). Agreements to work across government as well as infrastructure to monitor and survey risks can assist with stabilising the magnitude of risk going forwards. The Third National Adaptation Programme (NAP3) (Defra, 2024c), includes measures to safeguard food supply chains and food safety from climate disruptions. The programme is currently being implemented. The FSA, along with co-funders, is investing in the new UK Food Safety Network which aims to implement effective measures for enhancing food safety. A National Preparedness Report (National Preparedness Commission, 2025) highlights food contamination as one of the key risks on the National Risk Register. However, until recently little attention has been given to food resilience, with an overreliance on market forces to protect the UK from shocks, climate or other risks.
Measures to safeguard UK nutrient security have received less attention compared with adaptation measures to minimise the environmental impact on UK food systems. These latter measures include an emphasis on sustainable sources in government buying standards for food and catering services, or the UK’s national food-based dietary guidelines (Eatwell Guide) (OHID, 2024). Such guidelines encourage, for example, sustainable sources of fish and palm oil as well as eating seasonally. Many positive health outcomes are associated with sustainable dietary practices and if we were to meet current dietary guidelines it is highly likely we would also reduce the environmental impacts of diets (Springmann et al., 2020). For example, by lowering intakes of red and processed meats and substituting these with plant sources of protein or fruits and vegetables, this would reduce the risks of diet-related non-communicable diseases (e.g., blood pressure from lowering sodium/salt intakes), whilst simultaneously reducing the greenhouse gas emissions and land use change impacts associated with different livestock practices. Any future change to the nutritional content of food supplies or the availability and accessibility of food, due to climate change, however, would need to be more directly reflected in national nutrition risk assessments. This is especially the case to protect vulnerable or disadvantaged populations, which may have specific needs or already be at risk of poor diets and experiencing a disproportionately higher burden of diet-related poor health status or disease (e.g., overweight and obesity, diabetes, vascular conditions and certain cancers).
Assessment of the evidence base and evidence gaps
The Low confidence level for current risks represents the low certainty, high variability and many gaps in the available evidence linking climate change to food safety incidents and diet-related mortality and morbidity in the UK. There is also an urgent need to improve the available evidence in other areas, including the impact of climate change on aquaculture and wild fisheries, and the role of climate change as a cause of malnutrition in all its forms (undernutrition, micronutrient deficiency diseases, and overweight/obesity/diet-related non-communicable disease).
3.2.5.2 England
Assessment of current and future magnitude of risk
There is no additional evidence specific to England. Evidence for the UK (3.2.5.1) was used to assess this risk. Current and future risk was assessed as Medium as tens of thousands of people will be affected.
Level of preparedness for risk
The National Preparedness Commission report identified a lack of cohesion in food security policy and preparedness for food resilience in England from food shocks due to climate change or other factors (National Preparedness Commission, 2025). The report highlighted a complacency in being able to source sufficient food based on meeting energy needs (kcal per person per week), rather than considering food and nutrient security, and an overreliance on business to find alternative supply during periods of disruption. It also highlighted that the 2023 National Risk Register includes risks from contamination of food supply but does not consider risks to nutrient security. The FSA is expected to update its review of climate change impacts on food safety and security, in line with the newly released cross-departmental National Food Strategy for England (Defra, 2025a).
Evaluation of urgency score
The risk magnitude is assessed as Medium for present and future scenarios with Low confidence. The overall urgency is Further investigation.
Table 3.23: Urgency scores for H5 Risks to food safety and nutrition for England. Details of how the scores in this table were calculated are in the Methods Chapter.
| England | |||||||||
| H5 | Risks to food safety and nutrition. | ||||||||
| Present | 2030 | 2050 | 2080 | ||||||
| Central | High | Central | High | Low | Central | High | |||
| No adaptation | M • | M • | M • | M • | M • | M • | M • | M • | |
| With adaptation | M • | M • | M • | M • | M • | M • | M • | ||
| Urgency scores | FI | FI | FI | FI | |||||
| Overall urgency score | FI | ||||||||
3.2.5.3 Northern Ireland
Assessment of current and future magnitude of risk
Current and short-term future risk (2030s) is assessed to be Medium based on evidence for the UK with thousands of people affected. Northern Ireland has a higher proportional share of the most deprived areas in the UK. This is especially the case for health, with nearly 28% of areas in Northern Ireland ranked within the most deprived 10% by poor health across the UK (UKDI briefing upcoming). This could make Northern Ireland more vulnerable to many climate-related health risks, including nutrition and food safety risks, although this was not considered to be sufficient to move the current risk from Medium to High magnitude.
Level of preparedness for risk
The NI Food Strategy Framework Action Plan 2025-2027 (DAERA, 2024b) represents a whole of government approach to food, recognising the impact of climate change on food safety and nutrition. This action plan was developed in partnership with the Food Safety Agency in NI, who work closely with Safefood to promote food safety and nutrition across Northern Ireland (DAERA, 2025a).
A draft third Northern Ireland Climate Change Adaptation Programme (NICCAP3) (DAERA, 2025b) was released for consultation in Jun-Aug 2025 and includes food security actions to protect the economy, communities, and environment from climate change impacts in the near term. For example, it includes actions to become more resilient against food supply shocks, such as the disruption to transport and distribution from Storm Debi in 2023 (DAERA, 2025b).
Evaluation of urgency score
The risk magnitude is assessed as Medium for present and future scenarios with Low confidence. The overall urgency is Further Investigation.
Table 3.24: Urgency scores for H5 Risks to food safety and nutrition for Northern Ireland. Details of how the scores in this table were calculated are in the Methods Chapter.
| Northern Ireland | |||||||||
| H5 | Risks to food safety and nutrition. | ||||||||
| Present | 2030 | 2050 | 2080 | ||||||
| Central | High | Central | High | Low | Central | High | |||
| No adaptation | M • | M • | M • | M • | M • | M • | M • | M • | |
| With adaptation | M • | M • | M • | M • | M • | M • | M • | ||
| Urgency scores | FI | FI | FI | FI | |||||
| Overall urgency score | FI | ||||||||
3.2.5.4 Scotland
Assessment of current and future magnitude of risk
There is no additional evidence specific to Scotland. Evidence for the UK (3.2.5.1) was used to assess this risk. Current and future risk was assessed as Medium as thousands of people will be affected.
Level of preparedness for risk
Several policies have been introduced by the Scottish Government in support of farming and food production in Scotland. These include the Good Food Nation (Scotland) Act 2022 (Scottish Government, 2022) which aims to benefit wellbeing through ensuring access to good quality food, and the Vision for Agriculture which promotes sustainable farming practice and provides financial support for adaptation from 2025. The Agriculture Reform Programme also explores funding options to support farmers to reduce exposure to climate hazards. Scottish Government has introduced a Local Food Strategy to promote local supply of food and reduce barriers to a healthy diet among disadvantaged groups. These policies are helpful in safeguarding access to an affordable healthy diet in general, although they do not currently directly address the nutritional impact of climate change.
Scotland has also prioritised food production from sustainable food systems, for example with additional sampling for mycotoxins and monitoring the health of shellfish harvesting areas. It seems likely, but yet unconfirmed, that increased adoption of similar sustainable farming approaches will make food supply and nutritional quality more resilient to the impacts of climate change (Altieri et al., 2015).
Evaluation of urgency score
The risk magnitude is assessed as Medium for present and future scenarios with Low confidence. The overall urgency is Further Investigation.
Table 3.25: Urgency scores for H5 Risks to food safety and nutrition for Scotland. Details of how the scores in this table were calculated are in the Methods Chapter.
| Scotland | |||||||||
| H5 | Risks to food safety and nutrition. | ||||||||
| Present | 2030 | 2050 | 2080 | ||||||
| Central | High | Central | High | Low | Central | High | |||
| No adaptation | M • | M • | M • | M • | M • | M • | M • | M • | |
| With adaptation | M • | M • | M • | M • | M • | M • | M • | ||
| Urgency scores | FI | FI | FI | FI | |||||
| Overall urgency score | FI | ||||||||
3.2.5.5 Wales
Assessment of current and future magnitude of risk
There is no additional evidence specific to Wales. Evidence for the UK (3.2.5.1) was used to assess this risk. Current and future risk was assessed as Medium as thousands of people will be affected.
Level of preparedness for risk
The Wales Community Food Strategy (Welsh Government, 2025b) is designed to build healthier and more resilient food systems in Wales to make healthier food accessible to all. The strategy aligns with the Healthy Weight: Healthy Wales plan (Welsh Government, 2023a) and the Child Poverty Strategy (Welsh Government, 2024a), as well as focusing on local food partnerships and increasing public sector spending on Welsh food and suppliers.
Climate change impacts on food security (see N11) and nutrition are being explored through a Climate Change Health Impact Assessment (Public Health Wales, 2023b (HIA D1)). High levels of carbon dioxide are thought to have reduced the nutrient content on some crops in Wales (Public Health Wales, 2023b (HIA D1)).
Evaluation of urgency score
The risk magnitude is assessed as Medium for present and future scenarios with Low confidence. The overall urgency is Further investigation.
Table 3.26: Urgency scores for H5 Risks to food safety and nutrition for Wales. Details of how the scores in this table were calculated are in the Methods Chapter.
| Wales | |||||||||
| H5 | Risks to food safety and nutrition. | ||||||||
| Present | 2030 | 2050 | 2080 | ||||||
| Central | High | Central | High | Low | Central | High | |||
| No adaptation | M • | M • | M • | M • | M • | M • | M • | M • | |
| With adaptation | M • | M • | M • | M • | M • | M • | M • | ||
| Urgency scores | FI | FI | FI | FI | |||||
| Overall urgency score | FI | ||||||||
3.2.6 Risks to health and social care delivery – H6
The UK health system includes primary, secondary and tertiary care facilities which are coordinated by devolved national health services. The provision of social care has more complex governance, with public and private providers of services to support vulnerable groups, including children, adults and older persons in their own home, as well as in residential or nursing homes. Climate risks are known to disrupt health services, cause acute increases in demand, undermine access to services, affect the standard of service delivery (quality of care), impact health and social care staff, and disrupt supply chains. Climate change may also affect demand for health care through changes to infectious disease patterns and the exacerbation of symptoms for persons with chronic (non-communicable) diseases (NCDs).
Headlines
- Significant disruption to health delivery from flooding of all types will increase in the future.
- Overheating in health facilities is an increasing issue with significant impacts on the quality of care, patients and staff. Damage to infrastructure, including IT systems, has been significant.
- There is more evidence since CCRA3-IA-TR on overheating in care homes and the cost-effectiveness of active and passive cooling measures, as well as behaviour change in reducing negative impacts on health of residents.
- There has been some progress in developing adaptation planning at the hospital level, but there is a lack of investment and regulation to support adaptation in the health and social care sector.
| Table 3.27: Urgency scores for H6 Risks to health and social care delivery. Details of how the scores in this table were calculated are in the Methods Chapter. | |||||||
| ID | Risk | Present | 2030 | 2050 | 2080 | Urgency | |
| H6 | Risks to health and social care delivery | UK | H • • | M • • | H • • • | H • • | MAN |
| England | H • • | M • • | H • • • | H • • | MAN | ||
| Northern Ireland | M • • | M • • | M • • | H • • | MAN | ||
| Scotland | H • • | M • • | M • • | H • • | MAN | ||
| Wales | M • • | M • • | M • • | H • • | MAN | ||
3.2.6.1 Evidence relevant to the entire United Kingdom
Current and future drivers of risk
Climate risks disrupt health and social care delivery. The impacts of climate risks are compounded by the fragmentation of services and limited general resilience within local and regional systems. Climate risks are broadly the same across all countries in terms of impacts, with heat risks a greater issue in England and Wales.
The increased risk of flooding and storm events is likely to increase the disruption of health and social care service access and delivery (see risks BE2 and BE3 for more detailed information on regional impacts). Health and social care services are very reliant on critical infrastructure, including water and power supplies (see I1, I3 and I8), and emergency planning (BE8). The health system relies heavily upon domestic and international supply chains which are likely to be affected by climate change (E3). High indoor temperatures are increasingly affecting health and social care services (see H1 and BE1). There is an emerging risk from wildfires to health facilities. Currently, flooding, storms and heatwaves represent the biggest climate risks.
Assessment of current magnitude of risk
The magnitude of the current risk is High due to economic, social and health costs of disruption to health services from flooding and heatwaves, and other extreme weather. The economic costs of impacts (damage to infrastructure) and disruption to services are primarily considered within this assessment. It also considers costs to population health (in terms of damage to health from loss or poor quality of services), which falls in the hundreds of millions of pounds damage (economic) of foregone opportunities.
Heatwaves are associated with short term (acute) increases in health service demand (ambulance call outs, accident and emergency visits, and emergency hospital admissions) (Rizmie et al., 2022). Heat impacts cause increased emergency admissions for ‘high admission cost’ clinical conditions, such as kidney injury and dementia (Hajat et al. 2024). Unplanned care (e.g., from heat-related impacts) is significantly more expensive than planned care, especially for older people. Heat impacts may also cause delays in discharge of patients (Brooks et al., 2023).
Overheating in health facilities has caused the cancellation of inpatient and outpatient health services. During the heatwave in 2022, elective surgeries were cancelled because of staff shortages and overheating in surgical theatres in England (Picciochi et al., 2023)(POST, 2024). Overheating has been reported in a range of health service types, including antenatal care, outpatient services and inpatient wards.
The impact of heatwaves on equipment is increasing (e.g., failure of essential refrigeration systems including morgue facilities, IT systems, other equipment) leading to loss of services and loss of medicines (Brooks et al., 2023). Extreme high temperatures (40°C) in 2022 caused a critical incident due to the sustained loss of all clinical IT services at a large hospital (Guy’s and St Thomas’ NHS Foundation, 2023).
Occupational heat stress, staff discomfort, and absenteeism increase during hot weather. This causes significant impacts on staff wellbeing and service delivery (Brooks et al., 2023; Davey et al., 2024). A UK-wide survey found that more than 90% of respondents, mainly nurses, perceived that occupational heat strain impaired their performance, especially when using personal protective equipment, and 20% reported heat-related absenteeism (Davey et al., 2024).
High temperatures present a risk to social care delivery, both in care homes and in the community. A significant proportion of social care is delivered in the home, and also by informal or unpaid carers (Health and Social Care Committee, 2025). Climate change represents a range of risks to social care delivery at home (Young and Bergseng, 2020).
The climate risk to residents in care homes is well established, with an increase in research evidence on the prevalence and risks from overheating associated with high outdoor temperatures. Power outages during extreme heat further compound risks, especially for patients relying on cooling devices or refrigerated medications (Al-Marwani, 2023).
Flooding and extreme rainfall have also disrupted health and social care services through damage to equipment and buildings. Storm damage to health facility buildings is costly, may lead to the cancellation of services, and can require relocation or evacuation of inpatients. Damage by heavy rainfall events is made worse by the poor state of many hospital buildings.
Flooding and storm events prevent staff and patients from accessing health facilities. There have been several flood events that have damaged health and social care facilities, such as evacuation of a care home during Storm Babet in 2023, or major disruption to services. The July 2021 flooding at Whipps Cross hospital in London led to approximately 100 inpatients being evacuated, and a major incident was declared (Barts Health NHS Trust, 2021).
Health service delivery relies on significant domestic and international supply chains for medicines and consumables. Floods have caused disruption of domestic supply chains. Climate risks may impact blood safety and supply chains (Viennet et al., 2025). In 2012, flooding of the NHS Blood and Transplant Centre in Bristol caused national disruption of blood product (Sheridan, 2019). Heatwaves can also disrupt cold chains for the supply of medications and vaccines (see H1).
Assessment of future magnitude of risk
Flood projections indicate an increase in flood risk for health system assets, including hospitals, care homes, GP surgeries and emergency services (see BE2) (Sayers et al., 2020). The updated national flood and coastal risk assessment (Environment Agency, 2025) estimates that currently 26% of health facilities are at flood risk from multiple sources and that this risk will increase to 32% in the 2050s under 4 °C climate scenario (high emission RCP8.5 scenario from UKCP18).
Temperature projections (see State of the Climate) indicate an increased risk of overheating in health and social care buildings. A few studies have projected future indoor temperatures in hospitals and care homes (Gupta et al., 2021; Gupta R et al., 2021; Tsoulou et al., 2021) and these indicate significant increases in risk without effective adaptation. No new projections of overheating in health facilities have been published.
Level of preparedness for risk
The health and social care systems in the UK are devolved and also complex in terms of the multiple agencies delivering care. There are national regulators who are responsible for standards of care in hospitals, care homes and other related services. Local authorities are responsible for commissioning some community care services.
Adaptation action in the healthcare sector is challenged because of a widely noted ‘fragmentation between tertiary, primary and social care services’ (UKHSA and NHS England, 2021, 2025).
Common passive cooling strategies may not adequately mitigate overheating risk in care homes in the 2050s and 2080s (Gupta et al., 2021). Further research has shown that passive cooling measures and air conditioning can be cost-effective in a range of care home settings (Ibbetson et al., 2025). It is not currently possible to assess the implementation of active or passive cooling across the NHS Estate.
The National Health Service (NHS) and Greener NHS lead the NHS system transition (Huang et al., 2024). All NHS Trusts and Integrated Care Boards are required to produce Green Plans that describe their decarbonisation and adaptation planning. Green Plans should be approved by the organisation’s board or governing body (NHS England, 2025b). These commitments gained legislative footing with the Health and Care Act 2022 (HM Government, 2022).
Assessment of the evidence base and evidence gaps
Confidence is Medium as there are several sources of high-quality independent evidence for present risk. The Fourth Health and Climate Adaptation Report highlights key evidence gaps (NHS England, 2025a) that, if addressed, could strengthen climate resilience in the health sector to current and future risks. There is a need for greater evidence on cooling strategies and behaviour change in care home settings (Gupta et al., 2021).
3.2.6.2 England
Assessment of current and future magnitude of risk
Reports of incidents of flooding have increased. The NHS Estates dataset (ERIC) has reported on flooding incidents since 2021. Flooding incidents have increased 103% (from 176 to 358) (NHS England Digital 2024). An incident is defined as an event that has a significant impact on health service delivery. It’s worth noting that the events recorded in ERIC will under-estimate the true impact of flooding on health services.
Overheating in hospital buildings has also increased in recent years and is also recorded in ERIC (NHS England Digital, 2023, 2024). These data show a 53% increase in overheating incidents from 2016 to 2023-24, with a peak in 2022/2023 reflecting the extreme hot summers (NHS England Digital, 2023, 2024). Around 450 heat-related deaths were estimated in hospitals, and around 500 in care homes, in 2024 (UKHSA, 2025). During the July 2022 heatwave, cooling system failures at two data centres supporting London’s largest NHS trust led to major IT outages at Guy’s, St Thomas’, and Evelina London hospitals. This forced a temporary switch to paper-based systems, caused more than 100 treatment delays, including a missed organ transplant, and resulted in £1.4 million in additional costs. It also placed a significant strain on staff morale (Guy’s and St Thomas’ NHS Foundation, 2023).
Monitoring of a range of care home types has demonstrated high indoor temperatures and limitations in training of staff around heat risks (Gupta R et al., 2021). Monitoring of three care homes in England during the hot summer of 2019 found temperatures frequently exceeding 30 °C, which is well above indicative threshold of 26 °C (Gupta and Howard, 2022). A study in two London care homes showed that indoor temperatures frequently exceeded 26 °C, with newly built homes more likely to overheat (Tsoulou et al., 2021). Even during non-extreme summers, overheating still occurs but awareness of the level of risk is low among those managing care homes (Gupta et al., 2021; Gupta R et al., 2021).
The CLIMACARE project has quantified overheating risks in more than 50 care homes in England (Ibbetson et al., 2025). Modelling shows that building modifications and/or behaviour changes are cost-effective to reduce heat-related mortality across a range of care home types (Ibbetson et al., 2025).
There is concern that power failures present additional risk for heat impacts in care homes that rely on air conditioning. A study of three care home buildings during the 2022 heatwave found that indoor temperatures initially increased rapidly (up to 4 °C in an hour in the worst case), as the building fabric was warmer than the indoor air and most modelled bedrooms overheated (exceeding the Chartered Institute of Building Services Engineers (CIBSE) overheating threshold of 26 °C operative temperature) (Simpson et al., 2025).
Under all future warming scenarios, it is very likely that overheating in hospitals and care homes will increase. Building models provide robust evidence for the likelihood of future indoor temperature increases under a range of climate scenarios, with assumptions about adaptations in terms of building interventions.
There have been several studies that estimate future increases in indoor temperatures in care homes. Temperature projections indicate an increase of 6-10 °C compared to the monitored data from 2019 (Tsoulou et al., 2021). By 2050, in a high-emission scenario, it is expected that nearly all bedrooms could exceed 26 °C during summer (Tsoulou et al., 2023). For a 2080s high-emission scenario, indoor temperatures in two London care homes were projected to exceed 32 °C, with peak temperatures reaching up to 40 °C in some locations, particularly in the newer care home (Gupta et al., 2021).
Level of preparedness for risk
The Greener NHS initiative focuses on adjusting healthcare systems and infrastructure to operate effectively amidst climate change (NHS England, 2025d). Trusts and Integrated Care Boards (ICBs) are required to develop a Green Plan, which involves adaptation plans, under the Health and Care Act (2022). All NHS Trusts have had Green Plans in place since June 2022 (NHS England, 2022). Adaptation planning was strengthened in the recently published Green Plan Guidance (NHS England, 2025c). It is too early to evaluate the impacts of the Green Plans and the strategies within. The NHS has published its CCRA tool (NHS England, 2025e) for Trusts and ICBs to ascertain the climate change risks to their sites and services and a Climate Adaptation Framework (NHS England, 2025b) to support NHS organisations to adapt to climate change. ERIC (NHS England Estates Returns Information Collection) has now published data for 2023 on overheating incidents and flooding incidents.
The NHS published a Net Zero Building Standard in 2023 for new buildings and large retro-fits. The current version of the Net Zero Building Standard promotes passive cooling techniques and recommends a thermal comfort assessment to be carried out for all occupied spaces. NHS England has committed to strengthening adaptation within future iterations of the Net Zero Building Standard. Furthermore, climate adaptation planning is included within the NHS core standards for emergency preparedness, resilience and response guidance (NHS England, 2023). In addition, the UKHSA delivers the Adverse Weather and Health Plan (AWHP) for England and issues Weather Health Alerts (WHAs) including guidance for health and social care providers in England to deal with extremes of heat and cold; the WHAs are primarily aimed at the health and social care sector to support their business continuity and EPRR arrangements.
Evaluation of urgency scores
The magnitude of this risk is assessed as High for the current and future scenarios, based primarily on hundreds of heat-related deaths in care homes and hospitals. Whilst the evidence base on quantified impacts upon health service delivery remains fragmented, the limited evidence, coupled with available monitoring data, indicates an increasing risk in both current and future climates. The magnitude of the current risk has increased due to the impacts of recent extreme weather on services. UK healthcare expenditure in 2024 was approximately £317 billion, or 11.1% of gross domestic product (ONS, 2025). The score considers the economic costs of impacts (damage to infrastructure) as well as the costs to population health.
Table 3.28: Urgency scores for H6 Risks to health and social care delivery for England. Details of how the scores in this table were calculated are in the Methods Chapter.
| England | |||||||||
| H6 | Risks to health and social care delivery. | ||||||||
| Present | 2030 | 2050 | 2080 | ||||||
| Central | High | Central | High | Low | Central | High | |||
| No adaptation | H • • | H • • | H • • • | H • • | H • • • | H • • | H • • | H • • | |
| With adaptation | M • • | H • • | H • • • | H • • • | H • • | H • • | H • • • | ||
| Urgency scores | MAN | MAN | MAN | MAN | |||||
| Overall urgency score | MAN | ||||||||
3.2.6.3 Northern Ireland
Assessment of current and future magnitude of risk
There is limited research on heat impacts on hospitals in Northern Ireland and no mechanisms for reporting overheating. However, it is likely that negative impacts of high temperature on health service delivery have occurred. There are several reports on flooding and storm events causing damage to hospitals and health facilities in Northern Ireland. For example, Storm Ciaran in November 2023 caused flood damage at Ulster Hospital that caused a ward to be closed and patients moved (Belfast Live, 2023). The current risk magnitude is assessed as Medium as there are likely to be hundreds of deaths and hundreds of thousands of people affected. In the 2050s, risk remains Medium but increases in the 2080s to High.
High indoor temperatures have been reported in larger care homes in Northern Ireland, leading to discomfort among residents and care workers (Kennedy-Asser, 2022). There is enough evidence to assess a magnitude score for Northern Ireland based on information from England where care home settings are similar, although the climate is cooler in Northern Ireland.
Level of preparedness for risk
The latest version of the Northern Ireland Climate Change Adaptation Programme (2024-2029) has undergone public consultation and publication is forthcoming (DAERA, 2025b). There is currently no evidence to suggest the health system in Northern Ireland is required to publish climate change adaptation plans. In care settings, precautions including monitoring fluid intake and longer break time are recommended for both staff and residents (Kennedy-Asser, 2022).
Evaluation of urgency score
The risk magnitude is assessed as Medium for present and future scenarios, except the assessment of High for the low and central 2080s scenarios. The current risk magnitude is assessed as Medium as there are likely to be hundreds of deaths, thousands of major health impacts, and hundreds of thousands of people affected. The overall urgency is More action needed.
Table 3.29: Urgency scores for H6 Risks to health and social care delivery for Northern Ireland. Details of how the scores in this table were calculated are in the Methods Chapter.
| Northern Ireland | |||||||||
| H6 | Risks to health and social care delivery. | ||||||||
| Present | 2030 | 2050 | 2080 | ||||||
| Central | High | Central | High | Low | Central | High | |||
| No adaptation | M • • | M • • | M • • | M • • | M • • | H • • | H • • | M • • | |
| With adaptation | M • • | M • • | M • • | M • • | H • • | H • • | M • • | ||
| Urgency scores | MAN | MAN | MAN | MAN | |||||
| Overall urgency score | MAN | ||||||||
3.2.6.4 Scotland
Assessment of current and future magnitude of risk
Each NHS board in Scotland has identified risks that could impact their assets and service provision, recognising a total of 952 potential climate risks across all 22 NHS boards. The key climate risks identified by the NHS boards include “extended periods of hot weather”, “combined climatic effects”, and “flooding” (National Services Scotland, 2025). The current risk magnitude is assessed as Medium as there are likely to be hundreds of deaths, thousands of major health impacts, and hundreds of thousands of people affected. In the 2050s, risk remains Medium but increases in the 2080s to High.
Level of preparedness for risk
Both NHS Scotland (2022) and Public Health Scotland (2023) have climate emergency and sustainability strategies to 2026. In addition, the Health and Social Care Alliance Scotland are actively working on climate change and adapting the sector in Scotland. The Health and Social Care Academy calls for collaborative efforts from government, local authorities, health and social care partnerships, and care providers to address the sector’s contribution to and vulnerability to climate change.
A review by Young and Bergseng (2020) found that no local authorities considered climate risks within plans for delivering care at home.
Evaluation of urgency score
The current risk magnitude is assessed as High as there are likely to be tens of heat-related deaths in care homes and hospitals, based on interpreting the analysis for England, and comparisons with similar heat-mortality statistics from H1. In the 2030s and 2050s it remains High but has the potential to be Medium if hospitals and care homes implement adaptation measures. The overall urgency is More action needed.
Table 3.30: Urgency scores for H6 Risks to health and social care delivery for Scotland. Details of how the scores in this table were calculated are in the Methods Chapter.
| Scotland | |||||||||
| H6 | Risks to health and social care delivery. | ||||||||
| Present | 2030 | 2050 | 2080 | ||||||
| Central | High | Central | High | Low | Central | High | |||
| No adaptation | H • • | H • • | H • • | H • • | H • • | H • • | H • • | H • • | |
| With adaptation | M • • | M • • | M • • | M • • | H • • | H • • | H • • | ||
| Urgency scores | MAN | MAN | MAN | MAN | |||||
| Overall urgency score | MAN | ||||||||
3.2.6.5 Wales
Assessment of current and future magnitude of risk
The Climate Change in Wales: Health Impacts Report (2023) highlights several key risks for older people and children in care settings. Higher temperatures have been impacting on IT infrastructure, equipment and medicines, as well as workforce health (Public Health Wales, 2023d (HIA D7.1)).
Level of preparedness for risk
Wales has a health and social care climate emergency national programme (Welsh Government, 2025c). In response to CCRA3-IA TR, a toolkit was developed that recommended securing long-term funding to adapt hospitals and care homes, integrating adaptation actions into decarbonisation plans, and developing cross-sector approaches to address risks in the social care sector (Welsh Government, 2024d). The Welsh Government’s adoption of the Well-being of Future Generations (Wales) Act in 2015 may further support adaptation efforts in the health sector (Welsh Government, 2015b).
Evaluation of urgency score
The current risk magnitude is assessed as Medium as there are likely to be a few heat-related deaths in care homes and hospitals, based on interpreting the analysis for England, and comparisons with similar heat-mortality statistics from H1. In the 2050s, risk remains Medium but increases in the 2080s to High. Public Health Wales undertook a health impact assessment and assessed several risks in hospitals and care settings. The mechanisms of impact will be like those in England for which there is more direct evidence.
Table 3.31: Urgency scores for H6 Risks to health and social care delivery for Wales. Details of how the scores in this table were calculated are in the Methods Chapter.
| Wales | |||||||||
| H6 | Risks to health and social care delivery. | ||||||||
| Present | 2030 | 2050 | 2080 | ||||||
| Central | High | Central | High | Low | Central | High | |||
| No adaptation | M • • | M • • | M • • | M • • | M • • | H • • | H • • | H • • | |
| With adaptation | M • • | M • • | M • • | M • • | H • • | H • • | H • • | ||
| Urgency scores | MAN | MAN | MAN | MAN | |||||
| Overall urgency score | MAN | ||||||||
3.3 Interdependencies between risks
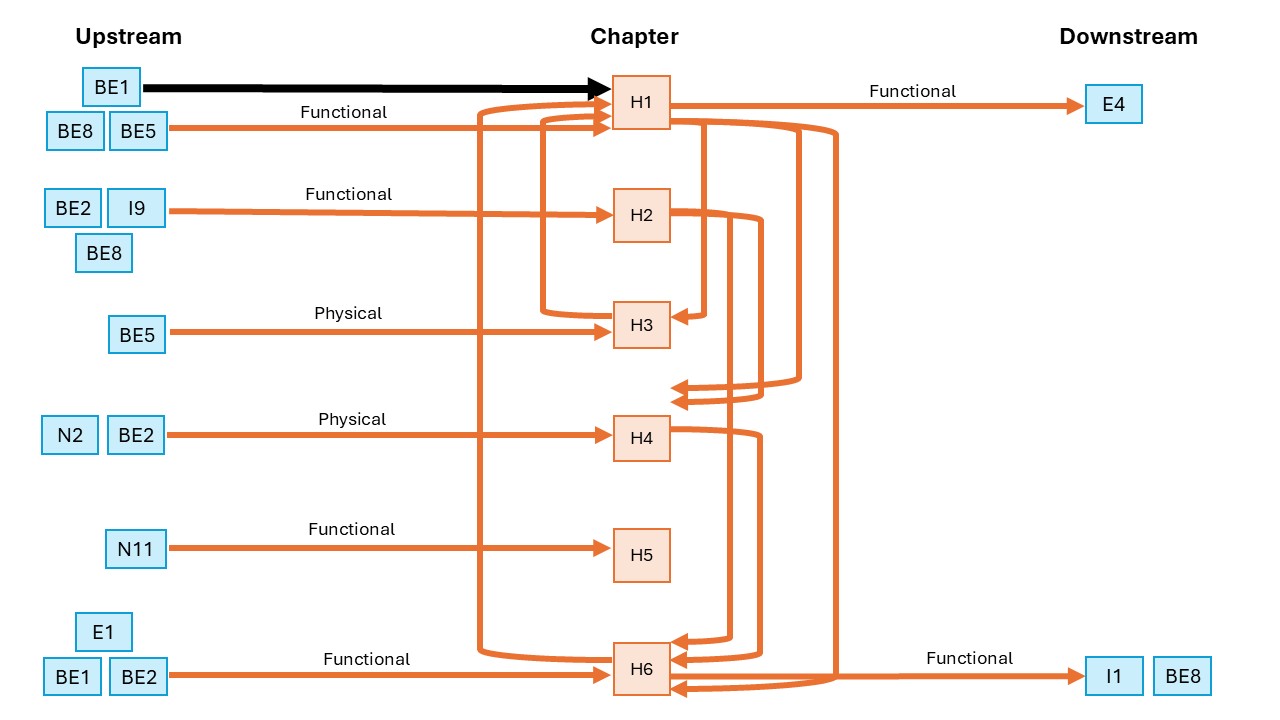
Heat-related illness (H1) can occur indoors and outdoors, with one of the leading causes of overheating in homes being due to building construction (BE1) and the quality of the indoor environments, including air quality (H3, BE5). Adaption measures such as urban forests can help reduce heat-mortality in built environments (BE1), but may create new spaces for vectors and infectious diseases (H4). During heatwaves, emergency services are at increased capacity, and health and social care facilities are put at risk through significant increases in heat-related illness, and disruptions to infrastructure, such as overheating IT (H6, BE8). The elderly and those in care homes are particularly at risk (H1, H6). The downstream impacts of heat illnesses can be a reduction in productivity through poor sleep, fatigue, and dehydration (E4), with further downstream impacts from overwhelmed health infrastructure impacting on the wider UK infrastructural systems (I1).
Water-related illness (H2) can be exacerbated by poor building design and location (BE2). Flooding episodes can hinder emergency services (BE8), and can increase waterborne infections (H4), especially when they overwhelm sewage systems (I9).
Risks to food safety and nutrition (H5) are closely linked to food security (N11), with both being put at higher risk due to heat-related illness and productivity (H1, E4).
3.4 References
Adams-Groom, B. et al. (2022) ‘Pollen season trends as markers of climate change impact: Betula, Quercus and Poaceae’, Science of The Total Environment, 831, pp. 154882–154882. Available at: https://doi.org/10.1016/J.SCITOTENV.2022.154882.
Agewall, S. et al. (2023) ‘SMALL-AREA ANALYSIS OF SHORT-TERM ASSOCIATIONTWEEN HEAT AND CARDIOVASCULAR MORTALITY IN FOUR EUROPEAN COUNTRIES’, Journal of the American College of Cardiology, 81(8), pp. 2114–2114. Available at: https://doi.org/10.1016/S0735-1097(23)02558-5.
Alari, A. et al. (2024) ‘Quantifying the Short-Term Mortality Effects of Wildfire Smoke in Europe: A Multi-Country Epidemiological Study in 654 Contiguous Regions’. Available at: https://doi.org/10.2139/SSRN.5068617.
Al-Marwani, S. (2023) ‘Climate change impact on the healthcare provided to patients’, Bulletin of the National Research Centre, 47(1), pp. 51–51. Available at: https://doi.org/10.1186/s42269-023-01026-9.
Altieri, M.A. et al. (2015) ‘Agroecology and the design of climate change-resilient farming systems’, Agronomy for Sustainable Development, 35(3), pp. 869–890. Available at: https://doi.org/10.1007/S13593-015-0285-2/FIGURES/3.
An, R. et al. (2020) ‘Projecting the Influence of Global Warming on Physical Activity Patterns: a Systematic Review’, Current Obesity Reports, 9(4), pp. 550–561. Available at: https://doi.org/10.1007/S13679-020-00406-W/METRICS.
Architecture & Design Scotland (2023) ‘Climate Ready School Grounds’. Available at: https://www.ads.org.uk/resource/climate-ready-school-grounds.
Arnell, N.W. et al. (2021) ‘Changing climate risk in the UK: A multi-sectoral analysis using policy-relevant indicators’, Climate Risk Management, 31, pp. 100265–100265. Available at: https://doi.org/10.1016/J.CRM.2020.100265.
Arulmukavarathan, A. et al. (2024) ‘Dengue in France in 2024 – A year of record numbers of imported and autochthonous cases’, New Microbes and New Infections, 62, pp. 101553–101553. Available at: https://doi.org/10.1016/J.NMNI.2024.101553.
Astell-Burt, T. and Feng, X. (2019) ‘Association of Urban Green Space With Mental Health and General Health Among Adults in Australia’, JAMA Network Open, 2(7), pp. e198209–e198209. Available at: https://doi.org/10.1001/JAMANETWORKOPEN.2019.8209.
Atchison, C.J. et al. (2009) ‘Temperature-dependent transmission of rotavirus in Great Britain and The Netherlands’, Proceedings of the Royal Society B: Biological Sciences, 277(1683), pp. 933–933. Available at: https://doi.org/10.1098/RSPB.2009.1755.
Atchison, C.J. et al. (2016) ‘Rapid Declines in Age Group–Specific Rotavirus Infection and Acute Gastroenteritis Among Vaccinated and Unvaccinated Individuals Within 1 Year of Rotavirus Vaccine Introduction in England and Wales’, The Journal of Infectious Diseases, 213(2), pp. 243–249. Available at: https://doi.org/10.1093/INFDIS/JIV398.
Augusto, S. et al. (2020) ‘Population exposure to particulate-matter and related mortality due to the Portuguese wildfires in October 2017 driven by storm Ophelia’, Environment International, 144, pp. 106056–106056. Available at: https://doi.org/10.1016/j.envint.2020.106056.
Autonomy Institute (2023) ‘Left out in the sun: work and high temperatures in the years ahead – The Autonomy Institute’, https://autonomy.work/ [Preprint]. Available at: https://autonomy.work/portfolio/left-out-in-the-sun/.
Baker-Austin, C. et al. (2017) ‘Non-Cholera Vibrios: The Microbial Barometer of Climate Change’, Trends in Microbiology, 25(1), pp. 76–84. Available at: https://doi.org/10.1016/j.tim.2016.09.008.
Barker, L.J. et al. (2024) ‘An appraisal of the severity of the 2022 drought and its impacts’, Weather, 79(7), pp. 208–219. Available at: https://doi.org/10.1002/WEA.4531.
Barts Health NHS Trust (2021) ‘Services affected by heavy rainfall’, www.bartshealth.nhs.uk [Preprint]. Available at: https://www.bartshealth.nhs.uk/news/services-affected-by-heavy-rainfall-11176/.
Bates, P.D. et al. (2023) ‘A climate-conditioned catastrophe risk model for UK flooding’, Natural Hazards and Earth System Sciences, 23(2), pp. 891–908. Available at: https://doi.org/10.5194/NHESS-23-891-2023.
van Bavel, B. et al. (2024) ‘Intersections between climate change and antimicrobial resistance: a systematic scoping review.’, The Lancet. Planetary health, 8(12), pp. e1118–e1128. Available at: https://doi.org/10.1016/S2542-5196(24)00273-0/ATTACHMENT/DA36D0D9-544D-41C9-B27C-6FAADE2FFC4C/MMC1.PDF.
BBC News (2024) Parasite outbreak cases in Devon double to 46. Available at: https://www.bbc.co.uk/news/articles/cx8q25qe484o (Accessed: 6 February 2026).
Belfast City Council (2024) Belfast City Council launches Northern Ireland’s first Local Area Energy Plan. Available at: https://www.belfastcity.gov.uk/news/belfast-city-council-launches-northern-ireland-s-f.
Bernard, P. et al. (2021) ‘Climate Change, Physical Activity and Sport: A Systematic Review’, Sports Medicine, 51(5), pp. 1041–1059. Available at: https://doi.org/10.1007/S40279-021-01439-4/METRICS.
Blöschl, G. et al. (2019) ‘Changing climate both increases and decreases European river floods’, Nature 2019 573:7772, 573(7772), pp. 108–111. Available at: https://doi.org/10.1038/s41586-019-1495-6.
Boyd, F. et al. (2018) ‘Who doesn’t visit natural environments for recreation and why: A population representative analysis of spatial, individual and temporal factors among adults in England’, Landscape and Urban Planning, 175, pp. 102–113. Available at: https://doi.org/10.1016/J.LANDURBPLAN.2018.03.016.
Brauer, M. et al. (2019) ‘Mortality–Air Pollution Associations in Low-Exposure Environments (MAPLE): Phase 1’, Research Reports: Health Effects Institute, 2019(203), pp. 203–203. Available at: https://pmc.ncbi.nlm.nih.gov/articles/PMC7334864/.
British Red Cross (2021) UK heatwave risk report. Available at: https://www.redcross.org.uk/about-us/what-we-do/we-speak-up-for-change/feeling-the-heat-a-british-red-cross-briefing-on-heatwaves-in-the-uk.
British Red Cross (2023) ‘Policy brief: public perception of heatwaves in the UK’, British Red Cross [Preprint]. Available at: https://www.redcross.org.uk/about-us/what-we-do/we-speak-up-for-change/policy-brief-public-perceptions-of-heatwaves-in-the-uk.
Brooks, K. et al. (2023) ‘Heatwaves, hospitals and health system resilience in England: a qualitative assessment of frontline perspectives from the hot summer of 2019’, BMJ Open, 13(3), pp. e068298–e068298. Available at: https://doi.org/10.1136/BMJOPEN-2022-068298.
Browning, M.H.E.M. et al. (2022) ‘Where greenspace matters most: A systematic review of urbanicity, greenspace, and physical health’, Landscape and Urban Planning, 217, pp. 104233–104233. Available at: https://doi.org/10.1016/j.landurbplan.2021.104233.
Bruce, R.C. et al. (2025) ‘Detection of West Nile virus via retrospective mosquito arbovirus surveillance, United Kingdom, 2025’, Eurosurveillance, 30(28), pp. 2500401–2500401. Available at: https://doi.org/10.2807/1560-7917.ES.2025.30.28.2500401;TIMESTAMP:1769788641616.
Bryan, K. et al. (2020) ‘The health and well-being effects of drought: assessing multi-stakeholder perspectives through narratives from the UK’, Climatic Change, 163(4), pp. 2073–2095. Available at: https://doi.org/10.1007/S10584-020-02916-X/FIGURES/4.
Büntgen, U. et al. (2022) ‘Plants in the UK flower a month earlier under recent warming’, Proceedings of the Royal Society B, 289(1968). Available at: https://doi.org/10.1098/RSPB.2021.2456.
Cabinet Office (2022) ‘The UK Government Resilience Framework’, www.gov.uk [Preprint]. Available at: https://www.gov.uk/government/publications/the-uk-government-resilience-framework.
Cabinet Office (2025a) ‘National Risk Register 2025’, www.gov.uk [Preprint]. Available at: https://www.gov.uk/government/publications/national-risk-register-2025.
Cabinet Office (2025b) ‘UK Biological Security Strategy Implementation Report June 2023 – June 2025’, www.gov.uk [Preprint]. Available at: https://www.gov.uk/government/publications/uk-biological-security-strategy-implementation-report-june-2023-june-2025/uk-biological-security-strategy-implementation-report-june-2023-june-2025-html#introduction.
Cai, Y. et al. (2020) ‘Prenatal, early-life, and childhood exposure to air pollution and lung function: The alspac cohort’, American Journal of Respiratory and Critical Care Medicine, 202(1), pp. 112–123. Available at: https://doi.org/10.1164/RCCM.201902-0286OC/SUPPL_FILE/DISCLOSURES.PDF.
Callaby, H. et al. (2025) ‘Tick-borne encephalitis: from tick surveillance to the first confirmed human cases, the United Kingdom, 2015 to 2023’, Eurosurveillance, 30(5), pp. 2400404–2400404. Available at: https://doi.org/10.2807/1560-7917.ES.2025.30.5.2400404.
Campbell, A.M., Willis, K. and Parsons, E. (2024) ‘Forecasting climate-associated non-tuberculous mycobacteria (NTM) infections in the UK using international surveillance data and machine learning’, PLOS Global Public Health, 4(8), pp. e0003262–e0003262. Available at: https://doi.org/10.1371/JOURNAL.PGPH.0003262.
Caryl, F. et al. (2025) ‘Urban park features and cardiovascular disease: a prospective analysis of 377,817 UK biobank participants’, Environment International, 206, p. 109913. Available at: https://doi.org/10.1016/j.envint.2025.109913.
Centre for Sustainable Healthcare (2026) NHS Forest, NHS Forest. Available at: https://nhsforest.org/ (Accessed: 5 February 2026).
Centre of Expertise for Waters (2024) ‘Building Public Health Resilience to Fluvial Flooding in Scotland’, https://www.crew.ac.uk [Preprint]. Available at: https://www.crew.ac.uk/publication/building-public-health-resilience.
Chang, K. et al. (2024) ‘Plant-based dietary patterns and ultra-processed food consumption: a cross-sectional analysis of the UK Biobank’, eClinicalMedicine, 78. Available at: https://doi.org/10.1016/j.eclinm.2024.102931.
Chauhan, S. et al. (2025) ‘Urban heat stress, air quality and climate change adaptation strategies in UK cities’, Frontiers of Engineering Management, 12(2), pp. 255–271. Available at: https://doi.org/10.1007/S42524-025-4029-Y/METRICS.
Chen, Y. et al. (2021) ‘Trimester effects of source-specific PM10 on birth weight outcomes in the Avon Longitudinal Study of Parents and Children (ALSPAC)’, Environmental Health: A Global Access Science Source, 20(1), pp. 1–12. Available at: https://doi.org/10.1186/S12940-020-00684-W/TABLES/4.
Cheng, X. et al. (2021) ‘A systematic review of evidence of additional health benefits from forest exposure’, Landscape and Urban Planning, 212, pp. 104123–104123. Available at: https://doi.org/10.1016/j.landurbplan.2021.104123.
Childs, M.L. et al. (2025) ‘Climate warming is expanding dengue burden in the Americas and Asia’, Proceedings of the National Academy of Sciences of the United States of America, 122(37), pp. e2512350122–e2512350122. Available at: https://doi.org/10.1073/PNAS.2512350122;WEBSITE:WEBSITE:PNAS-SITE;WGROUP:STRING:PUBLICATION.
Choubdar, N. et al. (2019) ‘Effect of Meteorological Factors on Hyalomma Species Composition and Their Host Preference, Seasonal Prevalence and Infection Status to Crimean-Congo Haemorrhagic Fever in Iran’, Journal of Arthropod-Borne Diseases, 13(3), pp. 268–283. Available at: https://pmc.ncbi.nlm.nih.gov/articles/PMC6928388/ (Accessed: 8 February 2026).
Clark, S.N. et al. (2023) ‘The Burden of Respiratory Disease from Formaldehyde, Damp and Mould in English Housing’, Environments – MDPI, 10(8), pp. 136–136. Available at: https://doi.org/10.3390/ENVIRONMENTS10080136/S1.
Climate Northern Ireland (2025) ‘NIAdapts Planning Toolkit’, https://www.niadapts.org.uk/ [Preprint]. Available at: https://www.niadapts.org.uk/.
Cole, R. et al. (2023) ‘The contribution of demographic changes to future heat-related health burdens under climate change scenarios’, Environment International, 173, pp. 107836–107836. Available at: https://doi.org/10.1016/J.ENVINT.2023.107836.
Cole, R. et al. (2024) ‘Systemic inequalities in heat risk for greater London’, Environment International, 190, pp. 108925–108925. Available at: https://doi.org/10.1016/J.ENVINT.2024.108925.
Colpitts, T.M. et al. (2012) ‘West Nile Virus: Biology, Transmission, and Human Infection’, Clinical Microbiology Reviews [Preprint]. Available at: https://doi.org/10.1128/CMR.00045-12.
COMEAP (2022) Air pollution: cognitive decline and dementia. Available at: https://www.gov.uk/government/publications/air-pollution-cognitive-decline-and-dementia.
Cox, E. (2021) ‘Resilience of the Future Energy System: Impacts of Energy Disruptions on Society UKERC Working Paper’, UK Energy Research Centre (UKERC) [Preprint].
Cruz, J. et al. (2020) ‘Effect of Extreme Weather Events on Mental Health: A Narrative Synthesis and Meta-Analysis for the UK’, International Journal of Environmental Research and Public Health 2020, Vol. 17, Page 8581, 17(22), pp. 8581–8581. Available at: https://doi.org/10.3390/IJERPH17228581.
Cull, B. et al. (2021) ‘A nationwide study on Borrelia burgdorferi s.l. infection rates in questing Ixodes ricinus: a six-year snapshot study in protected recreational areas in England and Wales’, Medical and Veterinary Entomology, 35(3), pp. 352–360. Available at: https://doi.org/10.1111/MVE.12503.
Cunningham, N. et al. (2024) ‘An outbreak of Shiga toxin-producing Escherichia coli (STEC) O157:H7 associated with contaminated lettuce and the cascading risks from climate change, the United Kingdom, August to September 2022’, Eurosurveillance, 29(36). Available at: https://doi.org/10.2807/1560-7917.ES.2024.29.36.2400161.
DAERA (2017) ‘The Water Environment (Water Framework Directive) Regulations (Northern Ireland) 2017’, www.legislation.gov.uk [Preprint].
DAERA (2019) Northern Ireland Climate Change Adaptation Programme 2019-2024. Department of Agriculture, Environment and Rural Affairs, NI. Available at: https://www.daera-ni.gov.uk/publications/northern-ireland-climate-change-adaptation-programme-2019-2024 (Accessed: 8 February 2026).
DAERA (2020) Clean Air Strategy for Northern Ireland A Public Discussion Document. Available at: https://www.daera-ni.gov.uk/sites/default/files/consultations/daera/20.21.066 Draft Clean Air Strategy for NI – Public Discussion Doc Final V6.PDF.
DAERA (2021) ‘Green Growth Strategy’, https://www.daera-ni.gov.uk [Preprint]. Available at: https://www.daera-ni.gov.uk/articles/green-growth-strategy.
DAERA (2024a) ‘Environmental Improvement Plan for Northern Ireland’, www.daera-ni.gov.uk [Preprint]. Available at: https://www.daera-ni.gov.uk/publications/environmental-improvement-plan-northern-ireland.
DAERA (2024b) ‘Northern Ireland Food Strategy Framework Action Plan 2025 – 2027’.
DAERA (2025a) Northern Ireland Food Strategy Framework Action Plan 2025-2027. Available at: https://www.daera-ni.gov.uk/publications/northern-ireland-food-strategy-framework-action-plan-2025-2027 (Accessed: 6 February 2026).
DAERA (2025b) ‘Public Consultation on the draft Third Northern Ireland Climate Change Adaptation Programme (NICCAP3)’. Available at: https://www.daera-ni.gov.uk/consultations/public-consultation-draft-third-northern-ireland-climate-change-adaptation-programme-niccap3.
Damtew, Y.T. et al. (2024) ‘The impact of temperature on non-typhoidal Salmonella and Campylobacter infections: an updated systematic review and meta-analysis of epidemiological evidence’, eBioMedicine, 109, pp. 105393–105393. Available at: https://doi.org/10.1016/J.EBIOM.2024.105393/ATTACHMENT/3C44233F-59AA-4AF7-8041-5A333EAC4A14/MMC1.DOCX.
Davey, S.L. et al. (2024) ‘Prevalence of occupational heat stress across the seasons and its management amongst healthcare professionals in the UK’, Applied Ergonomics, 118, pp. 104281–104281. Available at: https://doi.org/10.1016/J.APERGO.2024.104281.
DCMS (2025) ‘Exploring the financial implications of climate change on grassroots sport’, www.gov.uk [Preprint]. Available at: https://www.gov.uk/government/publications/exploring-the-financial-implications-of-climate-change-on-grassroots-sport/exploring-the-financial-implications-of-climate-change-on-grassroots-sport#executive-summary.
Defra (2019) ‘Clean Air Strategy 2019’, www.gov.uk [Preprint]. Available at: https://www.gov.uk/government/publications/clean-air-strategy-2019.
Defra (2022) Air quality PM2.5 targets Detailed evidence report. Available at: https://consult.defra.gov.uk/natural-environment-policy/consultation-on-environmental-targets/supporting_documents/Air quality targets Detailed Evidence report.pdf.
Defra (2023) Air quality strategy: framework for local authority delivery. UK Government. Available at: https://www.gov.uk/government/publications/the-air-quality-strategy-for-england/air-quality-strategy-framework-for-local-authority-delivery.
Defra (2024a) ‘Air Pollution in the UK 2023’, https://uk-air.defra.gov.uk/ [Preprint]. Available at: https://uk-air.defra.gov.uk/assets/documents/annualreport/air_pollution_uk_2023_issue_1.pdf.
Defra (2024b) ‘Preventing and Tackling Mental Ill Health through Green Social Prescribing Project Evaluation – BE0191’, https://sciencesearch.defra.gov.uk [Preprint]. Available at: https://sciencesearch.defra.gov.uk/ProjectDetails?ProjectId=20772.
Defra (2024c) Third National Adaptation Programme (NAP3). Available at: http://files/1103/Environment – 2023 – Third National Adaptation Programme.pdf.
Defra (2025a) A UK government food strategy for England, considering the wider UK food system. Defra. Available at: https://www.gov.uk/government/publications/a-uk-government-food-strategy-for-england/a-uk-government-food-strategy-for-england-considering-the-wider-uk-food-system (Accessed: 8 February 2026).
Defra (2025b) Environmental Improvement Plan 2025. Available at: https://www.gov.uk/government/publications/environmental-improvement-plan-2025 (Accessed: 5 February 2026).
Defra (2025c) Water (Special Measures) Act: policy statement. Available at: https://www.gov.uk/government/publications/water-special-measures-bill-policy-statement.
Defra (2025d) What is the Daily Air Quality Index?- Defra, UK. Available at: https://uk-air.defra.gov.uk/air-pollution/daqi?view=more-info.
Defra Air Quality Expert Group (AQEG) (2021) Ozone in the UK – Recent Trends and Future Projections. Available at: https://uk-air.defra.gov.uk/library/reports.php?report_id=1064.
Deguen, S. et al. (2021) ‘Are the effects of air pollution on birth weight modified by infant sex and neighborhood socioeconomic deprivation? A multilevel analysis in Paris (France)’, PLOS ONE, 16(4), pp. e0247699–e0247699. Available at: https://doi.org/10.1371/JOURNAL.PONE.0247699.
Delgado-Saborit, J.M. et al. (2024) ‘Assessment of the health impacts and costs associated with indoor nitrogen dioxide exposure related to gas cooking in the European Union and the United Kingdom’. Available at: http://hdl.handle.net/10234/692234.
Department for Infrastructure (2018) Northern Ireland Flood Risk Assessment (NIFRA) 2018. Available at: https://www.infrastructure-ni.gov.uk/publications/northern-ireland-flood-risk-assessment-nifra-2018 (Accessed: 6 February 2026).
Department of Finance (2023) ‘Consultation on a review of energy efficiency requirements and related areas of Building Regulations | Department of Finance’. Available at: https://www.finance-ni.gov.uk/consultations/consultation-review-energy-efficiency-requirements-and-related-areas-building-regulations.
DHSC CMO (2022) Chief Medical Officer’s annual report 2022: air pollution. Available at: https://www.gov.uk/government/publications/chief-medical-officers-annual-report-2022-air-pollution.
Dimitroulopoulou, C. (2012) ‘Ventilation in European dwellings: A review’, Building and Environment, 47(1), pp. 109–125. Available at: https://doi.org/10.1016/J.BUILDENV.2011.07.016.
Djennad, A. et al. (2019) ‘Seasonality and the effects of weather on Campylobacter infections’, BMC Infectious Diseases, 19(1), pp. 1–10. Available at: https://doi.org/10.1186/S12879-019-3840-7/FIGURES/4.
DLUHC (2024) ‘National Planning Policy Framework’, www.gov.uk [Preprint]. Available at: https://www.gov.uk/government/publications/national-planning-policy-framework–2.
Dodd, S. et al. (2024) ‘Health impacts of climate change in the UK: A qualitative synthesis detailing the conjuncture of social structure, extreme weather, and mental health’, SSM – Qualitative Research in Health, 6, pp. 100475–100475. Available at: https://doi.org/10.1016/J.SSMQR.2024.100475.
Dominici, F. et al. (2022) ‘Assessing Adverse Health Effects of Long-Term Exposure to Low Levels of Ambient Air Pollution: Implementation of Causal Inference Methods’, Research Reports: Health Effects Institute, 2022(211), pp. 211–211. Available at: https://pmc.ncbi.nlm.nih.gov/articles/PMC9530797/.
Donaldson (2006) ‘Climate change and the end of the respiratory syncytial virus season’, Clinical Infectious Diseases, 42(5), pp. 677–679. Available at: https://doi.org/10.1086/500208/3/M_42-5-677-FIG001.GIF.
{kind=link}
Ebi, K.L. et al. (2018) ‘Health risks of warming of 1.5 °C, 2 °C, and higher, above pre-industrial temperatures’, Environmental Research Letters, 13(6), pp. 063007–063007. Available at: https://doi.org/10.1088/1748-9326/AAC4BD.
ECDC (2025) ‘Shiga toxin-producing Escherichia coli (STEC)’, www.ecdc.europa.eu [Preprint]. Available at: https://www.ecdc.europa.eu/en/shiga-toxin-producing-escherichia-coli-stec.
eClinicalMedicine (2022) ‘Awaab Ishak and the politics of mould in the UK’, eClinicalMedicine, 54, pp. 101801–101801. Available at: https://doi.org/10.1016/J.ECLINM.2022.101801.
Eisenman, D.P. and Galway, L.P. (2022) ‘The mental health and well-being effects of wildfire smoke: a scoping review’, BMC Public Health, 22(1), pp. 1–17. Available at: https://doi.org/10.1186/S12889-022-14662-Z/FIGURES/2.
Ekele, J.U. et al. (2025) ‘Current impacts of elevated CO2 on crop nutritional quality: a review using wheat as a case study’, Stress Biology, 5(1), pp. 34–34. Available at: https://doi.org/10.1007/S44154-025-00217-W.
Elliot, A.J. et al. (2010) ‘Syndromic surveillance to assess the potential public health impact of the Icelandic volcanic ash plume across the United Kingdom, April 2010’, Eurosurveillance, 15(23), pp. 19583–19583. Available at: https://doi.org/10.2807/ESE.15.23.19583-EN/CITE/REFWORKS.
Elliot, A.J. et al. (2021) ‘Spike in asthma healthcare presentations in eastern england during june 2021: A retrospective observational study using syndromic surveillance data’, International Journal of Environmental Research and Public Health, 18(23). Available at: https://doi.org/10.3390/IJERPH182312353/S1.
Elliott, L.R. et al. (2019) ‘The effects of meteorological conditions and daylight on nature-based recreational physical activity in England’, Urban Forestry & Urban Greening, 42, pp. 39–50. Available at: https://doi.org/10.1016/J.UFUG.2019.05.005.
Energy & Climate Intelligence Unit (2025) ‘The impact of climate change on British farms and farmers’ mental health’, https://eciu.net [Preprint]. Available at: https://eciu.net/analysis/reports/2025/embargoed-the-impact-of-climate-change-on-british-farms-and-farmers-mental-health.
Environment Agency (2021) ‘A method for monetising the mental health costs of flooding’, GOV.UK [Preprint]. Available at: https://www.gov.uk/flood-and-coastal-erosion-risk-management-research-reports/a-method-for-monetising-the-mental-health-costs-of-flooding.
Environment Agency (2025) ‘National assessment of flood and coastal erosion risk in England 2024’, www.gov.uk [Preprint]. Available at: https://www.gov.uk/government/publications/national-assessment-of-flood-and-coastal-erosion-risk-in-england-2024/national-assessment-of-flood-and-coastal-erosion-risk-in-england-2024.
Environmental Audit Committee (2023) ‘Heat resilience and sustainable cooling, HC 1671 (Oral evidence)’.
Evangelopoulos, D. et al. (2022) Health Impact Assessment of Current and Past Air Pollution on Asthma in London. Available at: https://www.imperial.ac.uk/medicine/departments/school-public-health/environmental-research-group/research/air-pollution-epidemiology/air-pollution-and-asthma-in-london-2016-2019/.
Ewing, D.A. et al. (2021) ‘A novel approach for predicting risk of vector-borne disease establishment in marginal temperate environments under climate change: West Nile virus in the UK’, Journal of the Royal Society Interface, 18(178). Available at: https://doi.org/10.1098/RSIF.2021.0049.
Fahr, P. et al. (2025) ‘Quantifying the health-care burden of temperature in the National Health Service in England: an economic analysis of resource use and costs’, The Lancet. Planetary health, 9(12), pp. 101373–101373. Available at: https://doi.org/10.1016/j.lanplh.2025.101373.
Fanzo, J. et al. (2025) ‘Climate Change, Extreme Weather Events, Food Security, and Nutrition: Evolving Relationships and Critical Challenges’, Annual Review of Nutrition, 45(Volume 45, 2025), pp. 335–360. Available at: https://doi.org/10.1146/annurev-nutr-111324-111252.
Fenech, S. et al. (2021) ‘Future air pollution related health burdens associated with RCP emission changes in the UK’, Science of The Total Environment, 773, pp. 145635–145635. Available at: https://doi.org/10.1016/J.SCITOTENV.2021.145635.
Findlater, L. et al. (2023) ‘Help-seeking following a flooding event: a cross-sectional analysis of adults affected by flooding in England in winter 2013/14’, European Journal of Public Health, 33(5), pp. 834–840. Available at: https://doi.org/10.1093/EURPUB/CKAD082.
Finney, D.L. et al. (2018) ‘A projected decrease in lightning under climate change’, Nature Climate Change 2018 8:3, 8(3), pp. 210–213. Available at: https://doi.org/10.1038/s41558-018-0072-6.
Fischer, G., Hashmi, M. and Paterek, E. (2024) ‘Campylobacter Infection’, StatPearls [Preprint]. Available at: https://www.ncbi.nlm.nih.gov/books/NBK537033/.
Fleisher, J.M. et al. (1993) ‘Water and Non-Water-Related Risk Factors for Gastroenteritis among Bathers Exposed to Sewage-Contaminated Marine Waters’, International Journal of Epidemiology, 22(4), pp. 698–708. Available at: https://doi.org/10.1093/IJE/22.4.698.
Fleisher, J.M. et al. (1996) ‘Marine waters contaminated with domestic sewage: nonenteric illnesses associated with bather exposure in the United Kingdom’, American Journal of Public Health, 86(9), pp. 1228–1234. Available at: https://doi.org/10.2105/ajph.86.9.1228.
Fleisher, J.M. et al. (1998) ‘Estimates of the severity of illnesses associated with bathing in marine recreational waters contaminated with domestic sewage’, International Journal of Epidemiology, 27(4), pp. 722–726. Available at: https://doi.org/10.1093/IJE/27.4.722.
Fleisher, J.M. and Kay, D. (2006) ‘Risk perception bias, self-reporting of illness, and the validity of reported results in an epidemiologic study of recreational water associated illnesses’, Marine Pollution Bulletin, 52(3), pp. 264–268. Available at: https://doi.org/10.1016/j.marpolbul.2005.08.019.
Food Standards Agency (2023) ‘Food System Strategic Assessment: Trends and issues impacted by climate change/environmental factors’, www.food.gov.uk [Preprint]. Available at: https://www.food.gov.uk/research/food-system-strategic-assessment-trends-and-issues-impacted-by-climate-changeenvironmental-factors.
Food Standards Agency (2024) ‘What are the impacts of climate change, including society’s efforts to mitigate it and adapt to it, on the food system?’ Available at: https://www.food.gov.uk/research/climate-change.
Ford, C.L. et al. (2020) ‘Isolation and characterization of potentially pathogenic Vibrio species in a temperate, higher latitude hotspot’, Environmental Microbiology Reports, 12(4), pp. 424–434. Available at: https://doi.org/10.1111/1758-2229.12858.
Gandy, S.L., Hansford, K.M. and Medlock, J.M. (2023) ‘Possible expansion of Ixodes ricinus in the United Kingdom identified through the Tick Surveillance Scheme between 2013 and 2020’, Medical and Veterinary Entomology, 37(1), pp. 96–104. Available at: https://doi.org/10.1111/mve.12612.
Gao, J. et al. (2025) ‘The synergistic and mediating effects of ozone on associations between high temperature, heatwaves and mortality in the Greater London area between 2010 and 2018’, Environmental Research, 277, pp. 121577–121577. Available at: https://doi.org/10.1016/J.ENVRES.2025.121577.
Gasparrini, A. et al. (2022) ‘Small-area assessment of temperature-related mortality risks in England and Wales: a case time series analysis’, The Lancet Planetary Health, 6(7), pp. e557–e564. Available at: https://doi.org/10.1016/S2542-5196(22)00138-3.
GBD 2019 Diabetes and Air Pollution Collaborators et al. (2022) ‘Estimates, trends, and drivers of the global burden of type 2 diabetes attributable to PM2·5 air pollution, 1990–2019: an analysis of data from the Global Burden of Disease Study 2019’, The Lancet Planetary Health, 6(7), pp. e586–e600. Available at: https://doi.org/10.1016/S2542-5196(22)00122-X.
Geary, R.S. et al. (2023) ‘Green blue space exposure changes and impact on individual-level well-being and mental health: a population-wide dynamic longitudinal panel study with linked survey data’, Public Health Research, 11(10), pp. 1–176. Available at: https://doi.org/10.3310/LQPT9410.
Ghetu, C.C. et al. (2022) ‘Wildfire Impact on Indoor and Outdoor PAH Air Quality’, Environmental Science and Technology, 56(14), pp. 10042–10052. Available at: https://doi.org/10.1021/ACS.EST.2C00619/ASSET/IMAGES/LARGE/ES2C00619_0004.JPEG.
{kind=link}
Gillingham, E.L. et al. (2023) ‘Modelling the current and future temperature suitability of the UK for the vector Hyalomma marginatum (Acari: Ixodidae)’, Ticks and Tick-borne Diseases, 14(2), pp. 102112–102112. Available at: https://doi.org/10.1016/J.TTBDIS.2022.102112.
Godwin, J.L. et al. (2025) ‘Extreme heat impacts on daily life and adaptive behaviours captured through lived experience’, Environmental Research Letters, 20(5), p. 054077. Available at: https://doi.org/10.1088/1748-9326/adcbc5.
Gong, J., Part, C. and Hajat, S. (2022) ‘Current and future burdens of heat-related dementia hospital admissions in England’, Environment International, 159, pp. 107027–107027. Available at: https://doi.org/10.1016/j.envint.2021.107027.
Grange, S.K. et al. (2021) ‘COVID-19 lockdowns highlight a risk of increasing ozone pollution in European urban areas’, Atmospheric Chemistry and Physics, 21(5), pp. 4169–4185. Available at: https://doi.org/10.5194/ACP-21-4169-2021.
Greater London Authority (2025) ‘The Ultra Low Emission Zone (ULEZ) for London’, www.london.gov.uk [Preprint]. Available at: https://www.london.gov.uk/programmes-strategies/environment-and-climate-change/pollution-and-air-quality/ultra-low-emission-zone-ulez-london.
Green Alliance (2024) ‘Climate and health: Rising to the mental health challenge of climate change’, https://green-alliance.org.uk [Preprint].
Guercio, V. et al. (2021) ‘Exposure to indoor and outdoor air pollution from solid fuel combustion and respiratory outcomes in children in developed countries: a systematic review and meta-analysis’, Science of The Total Environment, 755, pp. 142187–142187. Available at: https://doi.org/10.1016/J.SCITOTENV.2020.142187.
Guercio, V., Doutsi, A. and Exley, K.S. (2022) ‘A systematic review on solid fuel combustion exposure and respiratory health in adults in Europe, USA, Canada, Australia and New Zealand’, International Journal of Hygiene and Environmental Health, 241, pp. 113926–113926. Available at: https://doi.org/10.1016/J.IJHEH.2022.113926.
Gulcebi, M.I. et al. (2025) ‘Imperatives and co-benefits of research into climate change and neurological disease’, Nature Reviews Neurology 2025 21:4, 21(4), pp. 216–228. Available at: https://doi.org/10.1038/s41582-024-01055-6.
Gupta R et al. (2021) ‘Examining the magnitude and perception of summertime overheating in London care homes’, Building Services Engineering Research and Technology, 42(6), pp. 653–675. Available at: https://doi.org/10.1177/01436244211013645/ASSET/IMAGES/LARGE/10.1177_01436244211013645-FIG7.JPEG.
{kind=link}
Gupta, R. et al. (2021) ‘Monitoring and modelling the risk of summertime overheating and passive solutions to avoid active cooling in London care homes’, Energy and Buildings, 252, pp. 111418–111418. Available at: https://doi.org/10.1016/J.ENBUILD.2021.111418.
Gupta, R. and Howard, A. (2022) ‘Summertime indoor temperatures and thermal comfort in nursing care homes in London’, 11th Windsor Conference: Resilient Comfort, WINDSOR 2020 – Proceedings, pp. 132–154. Available at: https://doi.org/10.4324/9781003244929-9/SUMMERTIME-INDOOR-TEMPERATURES-THERMAL-COMFORT-NURSING-CARE-HOMES-LONDON-RAJAT-GUPTA-ALASTAIR-HOWARD.
Guy’s and St Thomas’ NHS Foundation (2023) ‘Review of the Guy’s and St Thomas’ IT critical incident final report from the Deputy Chief Executive Officer, January 2023’, www.guysandstthomas.nhs.uk [Preprint]. Available at: https://www.guysandstthomas.nhs.uk/sites/default/files/2023-01/IT-critical-incident-review.pdf.
Hajat, S. et al. (2024) ‘Ambient heat and acute kidney injury: case-crossover analysis of 1 354 675 automated e-alert episodes linked to high-resolution climate data’, The Lancet Planetary Health, 8(3), pp. e156–e162. Available at: https://doi.org/10.1016/S2542-5196(24)00008-1.
Halios, C.H. et al. (2022) ‘Chemicals in European residences – Part I: A review of emissions, concentrations and health effects of volatile organic compounds (VOCs)’, Science of The Total Environment, 839, pp. 156201–156201. Available at: https://doi.org/10.1016/j.scitotenv.2022.156201.
Halsby, K.D. et al. (2014) ‘The relationship between meteorological variables and sporadic cases of Legionnaires’ disease in residents of England and Wales’, Epidemiology & Infection, 142(11), pp. 2352–2359. Available at: https://doi.org/10.1017/S0950268813003294.
Hanf, F.S. et al. (2025) ‘Towards a socio-ecological system understanding of urban flood risk and barriers to climate change adaptation using causal loop diagrams’, International Journal of Urban Sustainable Development, 17(1), pp. 69–102. Available at: https://doi.org/10.1080/19463138.2025.2474399;ISSUE:ISSUE:DOI.
Hanlon, H.M. et al. (2021) ‘Future changes to high impact weather in the UK’, Climatic Change, 166(3–4), pp. 1–23. Available at: https://doi.org/10.1007/S10584-021-03100-5/FIGURES/5.
Hansford, K.M. et al. (2026) ‘Mapping ticks (Acari: Argasidae, Ixodidae) and informing local public action: Insights from the United Kingdom Tick Surveillance Scheme (2021-2024)’, Ticks and Tick-borne Diseases, 17(1), p. 102579. Available at: https://doi.org/10.1016/j.ttbdis.2025.102579.
Harrison, J. et al. (2022) ‘The increased prevalence of Vibrio species and the first reporting of Vibrio jasicida and Vibrio rotiferianus at UK shellfish sites’, Water Research, 211, pp. 117942–117942. Available at: https://doi.org/10.1016/J.WATRES.2021.117942.
Hassall, R.M.J. et al. (2025) ‘Identifying hotspots and risk factors for tick-borne encephalitis virus emergence at its range margins to guide interventions, Great Britain’, Eurosurveillance, 30(13), pp. 2400441–2400441. Available at: https://doi.org/10.2807/1560-7917.ES.2025.30.13.2400441/CITE/REFWORKS.
Hawkes, F. et al. (2020) ‘Wetland mosquito survey handbook: assessing suitability of British wetlands for mosquitoes’. Natural Resources Institute. Available at: http://gala.gre.ac.uk/id/eprint/29851/ (Accessed: 8 February 2026).
Health and Social Care Committee (2025) ‘Health and Social Care Committee Adult Social Care Reform: the cost of inaction’, https://committees.parliament.uk [Preprint]. Available at: www.parliament.uk/copyright.
HM Government (2020) ‘The Air Quality (Domestic Solid Fuels Standards) (England) Regulations 2020’, www.legislation.gov.uk [Preprint]. Available at: https://www.legislation.gov.uk/uksi/2020/1095/contents/made.
HM Government (2021) ‘Environment Act 2021’, legislation.gov.uk [Preprint]. Available at: https://www.legislation.gov.uk/ukpga/2021/30/contents.
HM Government (2022) ‘Health and Care Act 2022’, www.legislation.gov.uk [Preprint]. Available at: https://www.legislation.gov.uk/ukpga/2022/31/contents.
HM Government (2023) ‘Levelling-up and Regeneration Act 2023’, www.legislation.gov.uk [Preprint]. Available at: https://www.legislation.gov.uk/ukpga/2023/55/contents.
Hoegh-Guldberg, O. et al. (2019) ‘The human imperative of stabilizing global climate change at 1.5°C’, Science, 365(6459). Available at: https://doi.org/10.1126/SCIENCE.AAW6974/SUPPL_FILE/AAW6974_HOEGH-GULDBERG_SM.PDF.
House of Commons Public Accounts Committee (2024) Government resilience: extreme weather. House of Commons. Available at: http://files/930/Government resilience extreme weather.pdf.
Howarth, C. (2024) ‘Preparing for heat risk is complex: Aligning adaptation and mitigation is essential’, PLOS Climate, 3(3), pp. e0000371–e0000371. Available at: https://doi.org/10.1371/JOURNAL.PCLM.0000371.
Huang, J. et al. (2024) ‘Mapping pedestrian heat stress in current and future heatwaves in Cardiff, Newport, and Wrexham in Wales, UK’, Building and Environment, 251, pp. 111168–111168. Available at: https://doi.org/10.1016/J.BUILDENV.2024.111168.
Huang, W.T.K. et al. (2020) ‘Weather regimes and patterns associated with temperature-related excess mortality in the UK: A pathway to sub-seasonal risk forecasting’, Environmental Research Letters, 15(12). Available at: https://doi.org/10.1088/1748-9326/ABCBBA.
Hunter, R.F. et al. (2019) ‘Environmental, health, wellbeing, social and equity effects of urban green space interventions: A meta-narrative evidence synthesis’, Environment International, 130, pp. 104923–104923. Available at: https://doi.org/10.1016/J.ENVINT.2019.104923.
Iacono, G.L. et al. (2024) ‘A mathematical, classical stratification modeling approach to disentangling the impact of weather on infectious diseases: A case study using spatio-temporally disaggregated Campylobacter surveillance data for England and Wales’, PLOS Computational Biology, 20(1), pp. e1011714–e1011714. Available at: https://doi.org/10.1371/JOURNAL.PCBI.1011714.
Ibbetson, A. et al. (2025) ‘Cost-benefit analysis of interventions to protect care home residents in England against heat risks’, Environmental Research: Health, 3(4), p. 045014. Available at: https://doi.org/10.1088/2752-5309/ae25c8.
Institute for Environmental Sciences (2024) Integrating Action on Air Quality & Climate Change: A Guide for Local Authorities. Available at: https://www.the-ies.org/resources/integrating-action-air-quality (Accessed: 6 February 2026).
Institute of Health Equity (2024) ‘Left out in the cold. The hidden health costs of cold homes’. Available at: https://www.instituteofhealthequity.org/resources-reports/left-out-in-the-cold-the-hidden-impact-of-cold-homes/copy-of-read-the-report.pdf.
Jackson, K. and Noushad, A. (2024) ‘The impacts of extreme temperature on mortality and emergency hospital admissions within East Sussex in comparison with pre-existing national trends’, Journal of Public Health, 46(1), pp. e23–e31. Available at: https://doi.org/10.1093/PUBMED/FDAD215.
Janssen, H. et al. (2023) ‘Cold indoor temperatures and their association with health and well-being: a systematic literature review’, Public Health, 224, pp. 185–194. Available at: https://doi.org/10.1016/J.PUHE.2023.09.006.
Jenkins, K. et al. (2022) ‘Updated projections of UK heat-related mortality using policy-relevant global warming levels and socio-economic scenarios’, Environmental Research Letters, 17(11), pp. 114036–114036. Available at: https://doi.org/10.1088/1748-9326/AC9CF3.
Johnston, C.J. et al. (2025) ‘Invasive mosquito surveillance in the United Kingdom 2020 to 2024: First detection of Aedes aegypti eggs in the UK and further detection of Aedes albopictus’, PLOS Global Public Health, 5(10), pp. e0004968–e0004968. Available at: https://doi.org/10.1371/JOURNAL.PGPH.0004968.
Kahraman, A. et al. (2022) ‘Contrasting future lightning stories across Europe’, Environmental Research Letters, 17(11), pp. 114023–114023. Available at: https://doi.org/10.1088/1748-9326/ac9b78.
Kay, A.L. et al. (2024) ‘Demonstrating the use of UNSEEN climate data for hydrological applications: Case studies for extreme floods and droughts in England’, Natural Hazards and Earth System Sciences, 24(9), pp. 2953–2970. Available at: https://doi.org/10.5194/NHESS-24-2953-2024.
Kay, D. et al. (1994) ‘Predicting likelihood of gastroenteritis from sea bathing: results from randomised exposure’, The Lancet, 344(8927), pp. 905–909. Available at: https://doi.org/10.1016/S0140-6736(94)92267-5.
Kendon, M. et al. (2024) ‘State of the UK Climate 2023’, International Journal of Climatology, 44(S1), pp. 1–117. Available at: https://doi.org/10.1002/JOC.8553;REQUESTEDJOURNAL:JOURNAL:10970088;JOURNAL:JOURNAL:10970088A;WGROUP:STRING:PUBLICATION.
Kennedy-Asser, A. (2022) ‘Castlederg. Care in weather extremes’. Available at: https://doi.org/10.17605/OSF.IO/9HMWD.
Kennedy-Asser, A.T. et al. (2025) ‘The role of local knowledge in enhancing climate change risk assessments in rural Northern Ireland’, Climate Risk Management, 48, pp. 100702–100702. Available at: https://doi.org/10.1016/j.crm.2025.100702.
Kent, C. et al. (2022) ‘Estimating unprecedented extremes in UK summer daily rainfall’, Environmental Research Letters, 17(1), pp. 14041–14041. Available at: https://doi.org/10.1088/1748-9326/AC42FB.
Kew, S.F. et al. (2024) ‘Autumn and Winter storms over UK and Ireland are becoming wetter due to climate change’. Available at: https://doi.org/10.25561/111577.
Konstantinoudis, G. et al. (2022) ‘Ambient heat exposure and COPD hospitalisations in England: a nationwide case-crossover study during 2007–2018’, Thorax, 77(11), pp. 1098–1104. Available at: https://doi.org/10.1136/thoraxjnl-2021-218374.
Kovats, R.S. et al. (2004) ‘The effect of temperature on food poisoning: a time-series analysis of salmonellosis in ten European countries’, Epidemiology & Infection, 132(3), pp. 443–453. Available at: https://doi.org/10.1017/S0950268804001992.
Kreusch, T.M. et al. (2019) ‘A probable case of tick-borne encephalitis (TBE) acquired in England, July 2019’, Eurosurveillance, 24(47), pp. 1900679–1900679. Available at: https://doi.org/10.2807/1560-7917.ES.2019.24.47.1900679.
Kuhn, K.G. et al. (2020) ‘Campylobacter infections expected to increase due to climate change in Northern Europe’, Scientific Reports 2020 10:1, 10(1), pp. 1–9. Available at: https://doi.org/10.1038/s41598-020-70593-y.
Kurganskiy, A. et al. (2021) ‘Predicting the severity of the grass pollen season and the effect of climate change in Northwest Europe’, Science Advances, 7(13), pp. 7658–7684. Available at: https://doi.org/10.1126/SCIADV.ABD7658/SUPPL_FILE/ABD7658_SM.PDF.
Lake et al. (2009) ‘A re-evaluation of the impact of temperature and climate change on foodborne illness’, Epidemiology & Infection, 137(11), pp. 1538–1547. Available at: https://doi.org/10.1017/S0950268809002477.
Lake, I. et al. (2019) ‘Exploring Campylobacter seasonality across Europe using The European Surveillance System (TESSy), 2008 to 2016’, Eurosurveillance, 24(13), p. 1800028. Available at: https://doi.org/10.2807/1560-7917.ES.2019.24.13.180028.
Lakhoo, D.P. et al. (2025) ‘A systematic review and meta-analysis of heat exposure impacts on maternal, fetal and neonatal health’, Nature Medicine, 31(2), pp. 684–694. Available at: https://doi.org/10.1038/s41591-024-03395-8.
Lam, H.C.Y. et al. (2024) ‘Association between ambient temperature and common allergenic pollen and fungal spores: A 52-year analysis in central England, United Kingdom’, Science of The Total Environment, 906, pp. 167607–167607. Available at: https://doi.org/10.1016/j.scitotenv.2023.167607.
Lee, A. et al. (2022) Fuel Poverty, Cold Homes and Health Inequalities in the UK. Available at: https://www.instituteofhealthequity.org/resources-reports/fuel-poverty-cold-homes-and-health-inequalities-in-the-uk.
Liu-Helmersson, J. et al. (2016) ‘Climate Change and Aedes Vectors: 21st Century Projections for Dengue Transmission in Europe’, eBioMedicine, 7, pp. 267–277. Available at: https://doi.org/10.1016/j.ebiom.2016.03.046.
Lopman, B. et al. (2009) ‘Host, Weather and Virological Factors Drive Norovirus Epidemiology: Time-Series Analysis of Laboratory Surveillance Data in England and Wales’, PLOS ONE, 4(8), pp. e6671–e6671. Available at: https://doi.org/10.1371/JOURNAL.PONE.0006671.
Louis, V.R. et al. (2005) ‘Temperature-driven campylobacter seasonality in England and Wales’, Applied and Environmental Microbiology, 71(1), pp. 85–92. Available at: https://doi.org/10.1128/AEM.71.1.85-92.2005/ASSET/268CA157-1366-4F1E-ABC7-72CE83FD79BC/ASSETS/GRAPHIC/ZAM0010550910005.JPEG.
{kind=link}
Macintyre, H.L. et al. (2023a) ‘Future impacts of O3 on respiratory hospital admission in the UK from current emissions policies’, Environment International, 178, pp. 108046–108046. Available at: https://doi.org/10.1016/j.envint.2023.108046.
Macintyre, H.L. et al. (2023b) ‘Impacts of emissions policies on future UK mortality burdens associated with air pollution’, Environment International, 174, pp. 107862–107862. Available at: https://doi.org/10.1016/j.envint.2023.107862.
Maggiore, A. et al. (2020) ‘Climate change and food safety Climate change as a driver of emerging risks for food and feed safety, plant, animal health and nutritional quality European Food Safety Authority (EFSA), Climate change and food safety’, EFSA Supporting Publications [Preprint]. Available at: https://doi.org/10.2903/sp.efsa.2020.EN-1881.
Manning, C. et al. (2024) ‘Compound wind and rainfall extremes: Drivers and future changes over the UK and Ireland’, Weather and Climate Extremes, 44, pp. 100673–100673. Available at: https://doi.org/10.1016/J.WACE.2024.100673.
Mansbridge, C.T. et al. (2022) ‘Autochthonous tick-borne encephalitis in the United Kingdom: A second probable human case and local eco-epidemiological findings’, Ticks and Tick-borne Diseases, 13(1), pp. 101853–101853. Available at: https://doi.org/10.1016/J.TTBDIS.2021.101853.
Marmot, M. et al. (2020) ‘Marmot Review 10 Years On – IHE’, The Institute of Health Equity [Preprint]. Available at: https://www.instituteofhealthequity.org/resources-reports/marmot-review-10-years-on.
Masselot, P. et al. (2023) ‘Excess mortality attributed to heat and cold: a health impact assessment study in 854 cities in Europe’, The Lancet Planetary Health, 7(4), pp. e271–e281. Available at: https://doi.org/10.1016/S2542-5196(23)00023-2.
Masselot, P. et al. (2025) ‘Estimating future heat-related and cold-related mortality under climate change, demographic and adaptation scenarios in 854 European cities’, Nature Medicine, pp. 1–9. Available at: https://doi.org/10.1038/s41591-024-03452-2.
Mbow, Cheikh et al. (2019) ‘Food security’, Climate Change and Land: An IPCC Special Report on climate change, desertification, land degradation, sustainable land management, food security, and greenhouse gas fluxes in terrestrial ecosystems, pp. 437–550. Available at: https://doi.org/10.1017/9781009157988.007.
McGinley, L. et al. (2021) ‘First report of human exposure to Hyalomma marginatum in England: Further evidence of a Hyalomma moulting event in north-western Europe?’, Ticks and Tick-borne Diseases, 12(1), pp. 101541–101541. Available at: https://doi.org/10.1016/J.TTBDIS.2020.101541.
McIver, L. et al. (2016) ‘Health Impacts of Climate Change in Pacific Island Countries: A Regional Assessment of Vulnerabilities and Adaptation Priorities’, Environmental Health Perspectives, 124(11), pp. 1707–1714. Available at: https://doi.org/10.1289/ehp.1509756.
Medlock, J.M. et al. (2017) ‘Detection of the invasive mosquito species Aedes albopictus in southern England’, The Lancet Infectious Diseases, 17(2), p. 140. Available at: https://doi.org/10.1016/S1473-3099(17)30024-5.
Medlock, J.M. et al. (2022) ‘Spatial and temporal heterogeneity of the density of Borrelia burgdorferi-infected Ixodes ricinus ticks across a landscape: A 5-year study in southern England’, Medical and Veterinary Entomology, 36(3), pp. 356–370. Available at: https://doi.org/10.1111/mve.12574.
MHCLG (2022) Ventilation: Approved Document F. Ministry for Housing Communities and Local Government. Available at: https://www.gov.uk/government/publications/ventilation-approved-document-f.
MHCLG, DHSC, and UKHSA (2024) ‘Understanding and addressing the health risks of damp and mould in the home’. Available at: https://www.gov.uk/government/publications/damp-and-mould-understanding-and-addressing-the-health-risks-for-rented-housing-providers/understanding-and-addressing-the-health-risks-of-damp-and-mould-in-the-home–2.
Ministry of Housing, C.& L.G. (2019) ‘Ventilation and indoor air quality in new homes’, www.gov.uk [Preprint]. Available at: https://www.gov.uk/government/publications/ventilation-and-indoor-air-quality-in-new-homes.
Ministry of Justice (2024) Climate change adaptation strategy 2024. UK Government. Available at: https://www.gov.uk/government/publications/climate-change-adaptation-strategy-moj/climate-change-adaptation-strategy-2024-moj.
Mitchell, D. et al. (2024) ‘Expert judgement reveals current and emerging UK climate-mortality burden’, The Lancet Planetary Health, 8(9), pp. e684–e694. Available at: https://doi.org/10.1016/S2542-5196(24)00175-X.
Mitchell, D. (2025) ‘Why we still don’t know the mounting health risks of climate change’, Nature, 637(8047), pp. 766–766. Available at: https://doi.org/10.1038/D41586-025-00149-5.
Mitsakou, C., Gowers, A. and Exley, K. (2022) Updated mortality burden estimates attributable to air pollution. Available at: https://assets.publishing.service.gov.uk/media/62ab19c4e90e07038e6df074/CHaPR_AQ_Special_Edition_2206116.pdf.
Mulchandani, R. et al. (2020) ‘The English National Cohort Study of Flooding & Health: Psychological morbidity at three years of follow up’, BMC Public Health, 20(1), pp. 1–7. Available at: https://doi.org/10.1186/S12889-020-8424-3/FIGURES/1.
Murage, P. et al. (2024) ‘Future temperature-related mortality in the UK under climate change scenarios: Impact of population ageing and bias-corrected climate projections’, Environmental Research, 259, pp. 119565–119565. Available at: https://doi.org/10.1016/j.envres.2024.119565.
Musacchio, A. et al. (2021) ‘Planning for the health impacts of climate change: Flooding, private groundwater contamination and waterborne infection – A cross-sectional study of risk perception, experience and behaviours in the Republic of Ireland’, Environmental Research, 194, pp. 110707–110707. Available at: https://doi.org/10.1016/J.ENVRES.2021.110707.
Myers, S.S. et al. (2014) ‘Increasing CO2 threatens human nutrition’, Nature, 510(7503), pp. 139–142. Available at: https://doi.org/10.1038/NATURE13179;SUBJMETA=106,2739,2807,694,704;KWRD=ENVIRONMENTAL+HEALTH.
Naghavi, M. et al. (2024) ‘Global burden of bacterial antimicrobial resistance 1990–2021: a systematic analysis with forecasts to 2050’, The Lancet, 404(10459), pp. 1199–1226. Available at: https://doi.org/10.1016/S0140-6736(24)01867-1.
National Preparedness Commission (2025) Just in Case: 7 steps to narrow the UK civil food resilience gap. Available at: https://nationalpreparednesscommission.uk/publications/just-in-case-7-steps-to-narrow-the-uk-civil-food-resilience-gap/ (Accessed: 8 February 2026).
National Services Scotland (2025) ‘NHS Scotland Climate Change Risk Assessments and Adaptation Plans: A Summary Report’, National Services Scotland [Preprint].
Natural England (2023) Green Infrastructure Framework. Natural England. Available at: https://designatedsites.naturalengland.org.uk/GreenInfrastructure/GIStandards.aspx.
Natural England (2025) ‘Natural England’s Strategy: Recovering Nature for Growth, Health and Security’, www.gov.uk [Preprint]. Available at: https://www.gov.uk/government/publications/natural-englands-strategy-recovering-nature-for-growth-health-and-security/natural-englands-strategy-recovering-nature-for-growth-health-and-security.
Natural Resources Wales (2023) ‘Flood Risk Management Plan: National overview’, www.naturalresources.wales [Preprint].
Natural Resources Wales (2025) Bathing water quality. Available at: https://naturalresources.wales/evidence-and-data/research-and-reports/water-reports/bathing-water-quality/?lang=en (Accessed: 8 February 2026).
Naumova, E.N. et al. (2005) ‘Effect of precipitation on seasonal variability in cryptosporidiosis recorded by the North West England surveillance system in 1990–1999’, Journal of Water and Health, 3(2), pp. 185–196. Available at: https://doi.org/10.2166/WH.2005.0017.
NHS (2023) ‘Legionnaires’ disease’, www.nhs.uk [Preprint]. Available at: https://www.nhs.uk/conditions/legionnaires-disease/.
NHS (2024) ‘Norovirus (vomiting bug)’, www.nhs.uk [Preprint]. Available at: https://www.nhs.uk/conditions/norovirus/.
NHS England (2025a) ‘4th Health and climate adaptation report’, https://www.england.nhs.uk [Preprint]. Available at: https://www.england.nhs.uk/long-read/4th-health-and-climate-adaptation-report/.
NHS England (2025b) ‘A climate adaptation framework for NHS organisations in England’, www.england.nhs.uk [Preprint]. Available at: https://www.england.nhs.uk/long-read/a-climate-adaptation-framework-for-nhs-organisations-in-england/.
NHS England (2025c) ‘Green plan guidance’, www.england.nhs.uk [Preprint]. Available at: https://www.england.nhs.uk/long-read/green-plan-guidance/.
NHS England (2025d) Greener NHS. Available at: https://www.england.nhs.uk/greenernhs/ (Accessed: 8 February 2026).
NHS England (2025e) NHS Climate Change Risk Assessment (CCRA) Tool. Available at: https://view.officeapps.live.com/op/view.aspx?src=https%3A%2F%2Fwww.england.nhs.uk%2Fwp-content%2Fuploads%2F2025%2F05%2Fprn01719-ii-nhs-climate-change-risk-assessment-tool.xlsm&wdOrigin=BROWSELINK (Accessed: 8 February 2026).
NHS England Digital (2023) Estates Returns Information Collection, Summary page and dataset for ERIC 2022/23. Available at: https://digital.nhs.uk/data-and-information/publications/statistical/estates-returns-information-collection/england-2022-23.
NHS England Digital (2024) Estates Returns Information Collection, Summary page and dataset for ERIC 2023/24. Available at: https://digital.nhs.uk/data-and-information/publications/statistical/estates-returns-information-collection/summary-page-and-dataset-for-eric-2023-24.
NHS Scotland (2022) NHS Scotland climate emergency and sustainability strategy: 2022-2026. Available at: https://www.gov.scot/publications/nhs-scotland-climate-emergency-sustainability-strategy-2022-2026/ (Accessed: 6 February 2026).
Nichols, G.L. et al. (2021) ‘Coronavirus seasonality, respiratory infections and weather’, BMC Infectious Diseases, 21(1), pp. 1–15. Available at: https://doi.org/10.1186/S12879-021-06785-2/FIGURES/4.
Nisa, H. and Mahase, E. (2025) ‘Boiling homes, blistering hospitals, a potential mental health crisis—UK is failing to prepare for climate emergency, expert warns’, BMJ, 391, pp. r2296–r2296. Available at: https://doi.org/10.1136/BMJ.R2296.
Northern Ireland Water (2023) ‘Climate Change Strategy’, www.niwater.com [Preprint]. Available at: https://www.niwater.com/climatechange/strategy/#downloads.
NPC, Reengage, and Disability Rights UK (2023) How will the climate and nature crises impact older people and Disabled people? A briefing for charities and funders, https://www.thinknpc.org/. Available at: https://www.thinknpc.org/resource-hub/everyones-environment-older-people-and-disabled-people/.
Nutsford, D., Pearson, A.L. and Kingham, S. (2013) ‘An ecological study investigating the association between access to urban green space and mental health’, Public Health, 127(11), pp. 1005–1011. Available at: https://doi.org/10.1016/J.PUHE.2013.08.016.
O’Donnell, E.C. and Thorne, C.R. (2020) ‘Drivers of future urban flood risk’, Philosophical Transactions of the Royal Society A, 378(2168). Available at: https://doi.org/10.1098/RSTA.2019.0216.
OHID (2024) The Eatwell Guide. www.gov.uk. Available at: https://www.gov.uk/government/publications/the-eatwell-guide (Accessed: 8 February 2026).
OHID (2025) ‘National Diet and Nutrition Survey 2019 2023: report’, www.gov.uk [Preprint]. Available at: https://www.gov.uk/government/statistics/national-diet-and-nutrition-survey-2019-to-2023/national-diet-and-nutrition-survey-2019-to-2023-report.
ONS (2020a) Coronavirus (COVID-19) related mortality rates and the effects of air pollution in England. Available at: https://www.ons.gov.uk/economy/environmentalaccounts/methodologies/coronaviruscovid19relatedmortalityratesandtheeffectsofairpollutioninengland.
ONS (2020b) Population estimates for the UK, England and Wales, Scotland and Northern Ireland. Available at: https://www.ons.gov.uk/peoplepopulationandcommunity/populationandmigration/populationestimates/bulletins/annualmidyearpopulationestimates/mid2019estimates.
ONS (2022) ‘Climate-related mortality and hospital admissions, England and Wales: 2001 to 2020’. Available at: https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/deaths/articles/climaterelatedmortalityandhospitaladmissionsenglandandwales/2001to2020.
ONS (2023) Winter mortality in England and Wales. Available at: https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/deaths/bulletins/excesswintermortalityinenglandandwales/2021to2022provisionaland2020to2021final.
ONS (2024) ‘Standards for official statistics on climate-health interactions’, www.ons.gov.uk [Preprint]. Available at: https://www.ons.gov.uk/aboutus/whatwedo/programmesandprojects/standardsforofficialstatisticsonclimatehealthinteractions.
ONS (2025) National Population Projections. Office for National Statistics. Available at: https://www.ons.gov.uk/peoplepopulationandcommunity/populationandmigration/populationprojections/datasets/2014basednationalpopulationprojectionstableofcontents.
Osborne, S. et al. (2021) ‘Air quality around schools: Part II – Mapping PM2.5 concentrations and inequality analysis’, Environmental Research, 197, pp. 111038–111038. Available at: https://doi.org/10.1016/j.envres.2021.111038.
Paavola, J. (2017) ‘Health impacts of climate change and health and social inequalities in the UK’, Environmental Health: A Global Access Science Source, 16(1), pp. 61–68. Available at: https://doi.org/10.1186/S12940-017-0328-Z/METRICS.
Pakdehi, M. et al. (2025) ‘Modeling the latent impacts of extreme floods on indoor mold spores in residential buildings: Application of machine learning algorithms’, Environment International, 196. Available at: https://doi.org/10.1016/j.envint.2025.109319.
Parker, E.R., Mo, J. and Goodman, R.S. (2022) ‘The dermatological manifestations of extreme weather events: A comprehensive review of skin disease and vulnerability’, The Journal of Climate Change and Health, 8, pp. 100162–100162. Available at: https://doi.org/10.1016/J.JOCLIM.2022.100162.
Parkin, J.G.H. et al. (2025) ‘Copper-enriched automotive brake wear particles perturb human alveolar cellular homeostasis’. Available at: https://doi.org/10.1186/s12989-024-00617-2.
Parry, S. et al. (2023) ‘Abrupt drought termination in the British–Irish Isles driven by high atmospheric vapour transport’, Environmental Research Letters, 18(10), p. 104050. Available at: https://doi.org/10.1088/1748-9326/acf145.
Petrou, G. et al. (2022) ‘Home energy efficiency under net zero: time to monitor UK indoor air’, BMJ (Clinical research ed.), 377, pp. e069435–e069435. Available at: https://doi.org/10.1136/BMJ-2021-069435.
Picciochi, M. et al. (2023) ‘Elective surgical services need to start planning for summer pressures’, British Journal of Surgery, 110(4), pp. 508–510. Available at: https://doi.org/10.1093/BJS/ZNAD033.
Price, R.H.M., Graham, C. and Ramalingam, S. (2019) ‘Association between viral seasonality and meteorological factors’, Scientific Reports 2019 9:1, 9(1), pp. 1–11. Available at: https://doi.org/10.1038/s41598-018-37481-y.
Public Health Scotland (2022) ‘Greenspace, Health and COVID-19’, www.publichealthscotland.scot [Preprint]. Available at: https://publichealthscotland.scot/our-blog/2022/july/greenspace-health-and-covid-19/.
Public Health Scotland (2023) PHS climate change and sustainability strategic plan. Available at: https://www.publichealthscotland.scot/publications/phs-climate-change-and-sustainability-strategic-plan/ (Accessed: 8 February 2026).
Public Health Scotland (2024) PHS adverse weather and health plan 2024–2027. Available at: https://www.publichealthscotland.scot/publications/phs-adverse-weather-and-health-plan-2024-2027/phs-adverse-weather-and-health-plan-2024-2027/.
Public Health Scotland (2025a) ‘Gastrointestinal and Zoonoses – Annual Report 2024’, https://publichealthscotland.scot/ [Preprint]. Available at: https://publichealthscotland.scot/publications/gastrointestinal-and-zoonoses/national-surveillance-of-gastrointestinal-infections-and-zoonoses-in-scotland/.
Public Health Scotland (2025b) ‘Heat impacts on health in Scotland’, https://publichealthscotland.scot [Preprint]. Available at: https://publichealthscotland.scot/publications/heat-impacts-on-health-in-scotland/heat-impacts-on-health-in-scotland-28-october-2025/.
Public Health Wales (2023a) ‘Climate Change in Wales: Health Impact Assessment’. Available at: https://phwwhocc.co.uk/wp-content/uploads/2023/07/PHW-Climate-Change-HIA-Summary-Report-English-Final-10_2023-002.pdf.
Public Health Wales (2023b) ‘Climate Change in Wales: Health Impact Assessment – D1 Food Security and Nutrition’, www.phwwhocc.co.uk [Preprint]. Available at: https://phwwhocc.co.uk/wp-content/uploads/2023/07/D1-Food-Security-and-Nutrition-Eng-final.pdf.
Public Health Wales (2023c) Climate Change in Wales: Health Impact Assessment – D5.3/P6.2 Flooding. Available at: https://phwwhocc.co.uk/wp-content/uploads/2023/07/D5.3P6.2-Flooding-Eng-final.pdf.
Public Health Wales (2023d) ‘Climate Change in Wales: Health Impact Assessment – D7.1 Health and social care services: access and delivery’.
Public Health Wales (2023e) ‘Private water supplies: An agile scope of the literature’, https://phw.nhs.wales/ [Preprint]. Available at: https://phw.nhs.wales/services-and-teams/observatory/evidence/evidence-documents/private-water-supplies-agile-scope/.
Public Health Wales (2025a) ‘Heat Morbidity Monitoring in Wales’, https://phw.nhs.wales/ [Preprint]. Available at: https://phw.nhs.wales/publications/publications1/heat-morbidity-monitoring-in-wales/.
Public Health Wales (2025b) ‘Heat Mortality Monitoring in Wales’, https://phw.nhs.wales [Preprint]. Available at: https://phw.nhs.wales/publications/publications1/heat-mortality-monitoring-in-wales/.
RCOG (2021) RCOG position statement Outdoor air pollution and pregnancy in the UK. Available at: https://www.rcog.org.uk/media/euxn0kya/outdoor-air-pollution-and-pregnancy-rcog-position-statement.pdf.
Rizmie, D. et al. (2022) ‘Impact of extreme temperatures on emergency hospital admissions by age and socio-economic deprivation in England’, Social Science & Medicine, 308, pp. 115193–115193. Available at: https://doi.org/10.1016/J.SOCSCIMED.2022.115193.
Royal College of Physicians (2025) ‘A breath of fresh air: responding to the health challenges of modern air pollution’, www.rcp.ac.uk [Preprint]. Available at: https://www.rcp.ac.uk/policy-and-campaigns/policy-documents/a-breath-of-fresh-air-responding-to-the-health-challenges-of-modern-air-pollution/.
Royal Society (2021) Effects of Net Zero Policies and Climate Change on Air Quality. Royal Society. Available at: https://royalsociety.org/-/media/policy/projects/air-quality/air-quality-and-climate-change-report.pdf.
Salm, L. et al. (2021) ‘How climate change interacts with inequity to affect nutrition’, WIREs Climate Change, 12(2), p. e696. Available at: https://doi.org/10.1002/wcc.696.
Sanderson, R.A. et al. (2018) ‘Spatio-temporal models to determine association between Campylobacter cases and environment’, International Journal of Epidemiology, 47(1), pp. 202–216. Available at: https://doi.org/10.1093/IJE/DYX217.
Sayers, P. et al. (2020) ‘Projections of Future Flood Risk – UK Climate Risk’, https://www.ukclimaterisk.org/publications/projections-of-future-flood-risk/ [Preprint]. Available at: https://www.ukclimaterisk.org/publications/projections-of-future-flood-risk/.
Sayers, P. et al. (2022) ‘Responding to climate change around England’s coast – The scale of the transformational challenge’, Ocean & Coastal Management, 225, pp. 106187–106187. Available at: https://doi.org/10.1016/J.OCECOAMAN.2022.106187.
Sayers, P., Penning-Rowsell, E.C. and Horritt, M. (2018) ‘Flood vulnerability, risk, and social disadvantage: current and future patterns in the UK’, Regional Environmental Change, 18(2), pp. 339–352. Available at: https://doi.org/10.1007/S10113-017-1252-Z/METRICS.
Scotland’s Environment (2022) ‘Impacts of summer heatwaves on air quality’, www.environment.gov.scot [Preprint]. Available at: https://www.environment.gov.scot/news/scotlands-environment-blog/impacts-of-summer-heatwaves-on-air-quality/.
Scottish Government (2021) Cleaner Air for Scotland 2 – Towards a Better Place for Everyone. Scottish Government. Available at: https://www.gov.scot/publications/cleaner-air-scotland-2-towards-better-place-everyone/.
Scottish Government (2022) ‘Good Food Nation (Scotland) Act 2022’. Available at: https://www.legislation.gov.uk/asp/2022/5/contents.
Scottish Government (2024a) National Flood Resilience Strategy. Available at: https://www.gov.scot/publications/national-flood-resilience-strategy-3/ (Accessed: 6 February 2026).
Scottish Government (2024b) ‘National Planning Framework 4’, www.gov.scot [Preprint].
Scottish Government (2024c) ‘Scottish National Adaptation Plan 2024-2029’, www.gov.scot [Preprint]. Available at: https://www.gov.scot/publications/scottish-national-adaptation-plan-2024-2029-2/pages/3/.
Scottish Government (2025a) ‘New Build Heat Standard’, www.gov.scot [Preprint]. Available at: https://www.gov.scot/publications/new-build-heat-standard-factsheet/.
Scottish Government (2025b) ‘Scottish National Adaptation Plan 2024-2029: monitoring and evaluation framework’, https://www.gov.scot/publications/ecosystem-restoration-code-engagement-paper/ [Preprint]. Available at: https://www.gov.scot/publications/scottish-national-adaptation-plan-2024-2029-monitoring-evaluation-framework/.
Scottish Water (2024) Scottish Water Climate Change Adaptation Plan 2024. Available at: https://www.scottishwater.co.uk/-/media/ScottishWater/Document-Hub/Key-Publications/Climate-Change/290224ScottishWaterAdaptationPlan.pdf (Accessed: 9 November 2024).
Seo, S. et al. (2019) ‘Association between urban green space and the risk of cardiovascular disease: A longitudinal study in seven Korean metropolitan areas’, Environment International, 125, pp. 51–57. Available at: https://doi.org/10.1016/J.ENVINT.2019.01.038.
Sharifi, A. et al. (2021) ‘A systematic review of the health co-benefits of urban climate change adaptation’, Sustainable Cities and Society, 74, pp. 103190–103190. Available at: https://doi.org/10.1016/j.scs.2021.103190.
Sheridan, K. (2019) ‘Hurricanes, droughts and wildfires: How biopharma is girding for climate change’, STAT [Preprint]. Available at: https://www.statnews.com/2019/02/15/hurricanes-droughts-and-wildfires-how-biopharma-is-girding-for-climate-change/.
Simpson, C.H. et al. (2025) ‘The mortality and associated economic burden of London’s summer urban heat island effect: a modelling study’, The Lancet Planetary Health, 9(3), pp. e219–e226. Available at: https://doi.org/10.1016/S2542-5196(25)00025-7.
Simpson, C.H., Brousse, O. and Heaviside, C. (2024) ‘Estimated mortality attributable to the urban heat island during the record-breaking 2022 heatwave in London’, Environmental Research Letters, 19(9), pp. 94047–94047. Available at: https://doi.org/10.1088/1748-9326/AD6C65.
Smith, R.B. et al. (2017) ‘Impact of London’s road traffic air and noise pollution on birth weight: retrospective population based cohort study’, BMJ, pp. j5299–j5299. Available at: https://doi.org/10.1136/bmj.j5299.
Snell, C., Bevan, M. and Thomson, H. (2015) ‘Justice, fuel poverty and disabled people in England’, Energy Research & Social Science, 10, pp. 123–132. Available at: https://doi.org/10.1016/J.ERSS.2015.07.012.
Springmann, M. et al. (2020) ‘The healthiness and sustainability of national and global food based dietary guidelines: modelling study’. Available at: https://doi.org/10.1136/bmj.m2322.
Stafoggia, M. et al. (2022) ‘Long-term exposure to low ambient air pollution concentrations and mortality among 28 million people: results from seven large European cohorts within the ELAPSE project’, The Lancet Planetary Health, 6(1), pp. e9–e18. Available at: https://doi.org/10.1016/S2542-5196(21)00277-1.
Stafoggia, M. et al. (2023) ‘Joint effect of heat and air pollution on mortality in 620 cities of 36 countries’, Environment International, 181, pp. 108258–108258. Available at: https://doi.org/10.1016/j.envint.2023.108258.
Stewart, C.G., Mahesh, A. and Mulvenna, C. (2024) ‘Thunderstorm asthma: a paediatric emergency department experience in London’, BMJ Paediatrics Open, 8(1), pp. 2572–2572. Available at: https://doi.org/10.1136/BMJPO-2024-002572.
Stirling, E.L. et al. (2020) ‘Quantifying the transboundary contribution of nitrogen oxides to UK air quality’, Atmospheric Science Letters, 21(2), pp. e955–e955. Available at: https://doi.org/10.1002/asl.955.
Talbot, C.J. et al. (2018) ‘The impact of flooding on aquatic ecosystem services’, Biogeochemistry 2018 141:3, 141(3), pp. 439–461. Available at: https://doi.org/10.1007/S10533-018-0449-7.
Tam, C.C. et al. (2006) ‘Temperature dependence of reported Campylobacter infection in England, 1989–1999’, Epidemiology & Infection, 134(1), pp. 119–125. Available at: https://doi.org/10.1017/S0950268805004899.
Taylor, J. et al. (2024) ‘The potential of urban trees to reduce heat-related mortality in London’, Environmental Research Letters, 19(5), pp. 054004–054004. Available at: https://doi.org/10.1088/1748-9326/AD3A7E.
The Guardian (2024) ‘“It brings back memories of Aberfan”: coal tip collapse in storms sparks revolt in Welsh valley’, www.theguardian.com [Preprint]. Available at: https://www.theguardian.com/uk-news/2024/nov/30/aberfan-welsh-valley-coal-tip-labour-reform-uk-storms?utm_source=chatgpt.com.
Thompson, R. et al. (2024) ‘Identification of individual-level clinical factors associated with increased risk of death during heatwaves: a time-stratified case-crossover study using national primary care records in England’, BMJ Public Health, 2(1), pp. e000927–e000927. Available at: https://doi.org/10.1136/BMJPH-2024-000927.
Thompson, R. et al. (2025) ‘Social determinants of heat-related mortality in England: a time-stratified case-crossover study using primary care records’, BMJ Public Health, 3(2), pp. e001111–e001111. Available at: https://doi.org/10.1136/BMJPH-2024-001111.
Transport for Wales (2023) Climate adaptation and resilience plan. Available at: https://tfw.wales/sites/default/files/2023-05/CARP_ENG.pdf.
Transport Scotland (2020) ‘National Transport Strategy 2’. Available at: https://www.transport.gov.scot/publication/national-transport-strategy-2/.
Trinanes, J. and Martinez-Urtaza, J. (2021) ‘Future scenarios of risk of Vibrio infections in a warming planet: a global mapping study’, The Lancet Planetary Health, 5(7), pp. e426–e435. Available at: https://doi.org/10.1016/S2542-5196(21)00169-8.
Tsoulou, I. et al. (2021) ‘Assessing the current and future risk of overheating in London’s care homes: The effect of passive ventilation’, Building Simulation Conference Proceedings, 17, pp. 2650–2657. Available at: https://doi.org/10.26868/25222708.2021.30677.
Tsoulou, I. et al. (2023) ‘Indoor environmental quality trade-offs due to summertime natural ventilation in London care homes’, Journal of Physics: Conference Series, 2600(9), pp. 092013–092013. Available at: https://doi.org/10.1088/1742-6596/2600/9/092013.
Twigg, M.M. et al. (2016) ‘Impacts of the 2014–2015 Holuhraun eruption on the UK atmosphere’, Atmospheric Chemistry and Physics, 16(17), pp. 11415–11431. Available at: https://doi.org/10.5194/acp-16-11415-2016.
UK Government (2010) ‘Flood and Water Management Act 2010’, legislation.gov.uk [Preprint]. Available at: https://www.legislation.gov.uk/ukpga/2010/29/contents.
UK100 (2023) ‘Local leading the way on integrating Clean Air and Net Zero’, www.uk100.org [Preprint]. Available at: https://www.uk100.org/publications/what-canz-be-done-local-authorities-leading-way-integrating-clean-air-and-net-zero.
UKHSA (2022) ‘Thunderstorm asthma and public health – looking back to move forward’, www.gov.uk [Preprint]. Available at: https://ukhsa.blog.gov.uk/2022/03/18/thunderstorm-asthma-and-public-health-looking-back-to-move-forward/.
UKHSA (2023) UKHSA strategic plan 2023 to 2026: executive summary. Available at: https://www.gov.uk/government/publications/ukhsa-strategic-plan-2023-to-2026/ukhsa-strategic-plan-2023-to-2026-executive-summary.
UKHSA (2024a) Health Effects of Climate Change (HECC) in the UK: 2023 report. Chapter 5: Impact of climate change policies on indoor environmental quality and health in UK housing. Available at: https://assets.publishing.service.gov.uk/media/65704f719462260721c569ca/HECC-report-2023-chapter-5-indoor-air-quality.pdf.
UKHSA (2024b) Health Effects of Climate Change (HECC) in the UK: 2023 report. Chapter 6: Outdoor airborne allergenic pollen and fungal spores. Available at: https://assets.publishing.service.gov.uk/media/6570509d3831ec0013c7496e/HECC-report-2023-chapter-6-aeroallergens.pdf.
UKHSA (2024c) Health Effects of Climate Change (HECC) in the UK: 2023 report. Chapter 7: Effect of climate change on infectious diseases in the UK. GOV.UK. Available at: https://assets.publishing.service.gov.uk/media/657087777469300012488921/HECC-report-2023-chapter-7-infectious-diseases.pdf.
UKHSA (2024d) Health Effects of Climate Change (HECC) in the UK: 2023 report. Chapter 8: Direct and indirect effects of climate change on vector. Available at: https://assets.publishing.service.gov.uk/media/65708af2809bc3001330819c/HECC-report-2023-chapter-8-vector-borne-diseases.pdf.
UKHSA (2024e) Health Effects of Climate Change (HECC) in the UK: 2023 report. Chapter 2: Temperature effects on mortality in a changing climate.
UKHSA (2024f) Health Effects of Climate Change (HECC) in the UK: 2023 report. Chapter 3: Climate change, flooding, coastal change and public health. Available at: https://www.gov.uk/government/publications/climate-change-health-effects-in-the-uk#:~:text=Chapter%203%3A%20Climate%20change,%20flooding%20and%20public%20health.
UKHSA (2024g) Health Effects of Climate Change (HECC) in the UK: 2023 report. Chapter 4: Impacts of climate change and policy on air pollution and human health. Available at: https://www.gov.uk/government/publications/climate-change-health-effects-in-the-uk.
UKHSA (2024h) Health Effects of Climate Change (HECC) in the UK: 2023 report. Chapter 9: Climate change and food supply. UKHSA. Available at: https://assets.publishing.service.gov.uk/media/659ff76ee96df5000df844c3/HECC-report-2023-chapter-9-food-supply.pdf.
UKHSA (2024i) Health Effects of Climate Change (HECC) in the UK: 2023 report. Chapter 10: Wildfires and health. Available at: https://assets.publishing.service.gov.uk/media/65705b7a7391350013b03bbc/HECC-report-2023-chapter-10-wildfires.pdf.
UKHSA (2024j) Health Effects of Climate Change (HECC) in the UK: 2023 report. Chapter 11: The direct and indirect effects of drought on human health in the UK.
UKHSA (2024k) Heat mortality monitoring report: 2023. GOV.UK. Available at: https://www.gov.uk/government/publications/heat-mortality-monitoring-reports/heat-mortality-monitoring-report-2023.
UKHSA (2024l) ‘Malaria imported into the UK: 2023’, www.gov.uk [Preprint]. Available at: https://www.gov.uk/government/publications/malaria-in-the-uk-annual-report/malaria-imported-into-the-uk-2023.
UKHSA (2024m) ‘Tick bite risks and prevention of Lyme disease: resources’, www.gov.uk [Preprint]. Available at: https://www.gov.uk/government/publications/tick-bite-risks-and-prevention-of-lyme-disease.
UKHSA (2024n) ‘What is cryptosporidium, and how can you avoid it in the water or on the farm?’, https://ukhsa.blog.gov.uk [Preprint]. Available at: https://ukhsa.blog.gov.uk/2024/05/17/what-is-cryptosporidium-and-how-can-you-avoid-it-in-the-water-or-on-the-farm/.
UKHSA (2025a) Adverse Weather and Health Plan. Available at: https://www.gov.uk/government/publications/adverse-weather-and-health-plan.
UKHSA (2025b) ‘Communicable disease outbreak management guidance: principles to support local health protection systems’, www.gov.uk [Preprint]. Available at: https://www.gov.uk/government/publications/communicable-disease-outbreak-management-guidance/communicable-disease-outbreak-management-guidance-principles-to-support-local-health-protection-systems.
UKHSA (2025c) Heat mortality monitoring report: 2022. Available at: https://www.gov.uk/government/publications/heat-mortality-monitoring-reports/heat-mortality-monitoring-report-2022.
UKHSA (2025d) ‘Heat mortality monitoring report, England: 2024’. Available at: https://www.gov.uk/government/statistics/heat-mortality-monitoring-report-england-2024/heat-mortality-monitoring-report-england-2024.
UKHSA (2025e) ‘Human Animal Infections and Risk Surveillance group (HAIRS)’, www.gov.uk [Preprint]. Available at: https://www.gov.uk/government/collections/human-animal-infections-and-risk-surveillance-group-hairs.
UKHSA (2025f) ‘Preparedness plan’, www.gov.uk [Preprint]. Available at: https://www.gov.uk/government/publications/emergency-preparedness-resilience-and-response-concept-of-operations/preparedness-plan.
UKHSA (2025g) ‘Priority pathogen families research and development tool’, www.gov.uk [Preprint]. Available at: https://www.gov.uk/government/publications/priority-pathogen-families-research-and-development-tool.
UKHSA, Defra, and DHSC (2020) ‘National contingency plan for invasive mosquitoes’, www.gov.uk [Preprint]. Available at: https://www.gov.uk/government/publications/national-contingency-plan-for-invasive-mosquitoes.
Vanoli, J. et al. (2024) ‘Association between long-term exposure to low ambient PM2.5 and cardiovascular hospital admissions: A UK Biobank study’, Environment International, 192, pp. 109011–109011. Available at: https://doi.org/10.1016/J.ENVINT.2024.109011.
Vaux, A.G.C. et al. (2019) ‘The challenge of invasive mosquito vectors in the U.K. during 2016–2018: a summary of the surveillance and control of Aedes albopictus’, Medical and Veterinary Entomology, 33(4), pp. 443–452. Available at: https://doi.org/10.1111/mve.12396.
Vaux, A.G.C. et al. (2021) ‘Identification, surveillance and management of Aedes vexans in a flooded river valley in Nottinghamshire, United Kingdom’, Journal of the European Mosquito Control Association, 39(1), pp. 15–25. Available at: https://doi.org/10.52004/JEMCA2021.0001.
Vaux, A.G.C. et al. (2024) ‘An update on the ecology, seasonality and distribution of Culex modestus in England’, Journal of the European Mosquito Control Association, 42(2), pp. 77–95. Available at: https://doi.org/10.52004/JEMCA20231003.
Vezzulli, L. et al. (2016) ‘Climate influence on Vibrio and associated human diseases during the past half-century in the coastal North Atlantic’, Proceedings of the National Academy of Sciences of the United States of America, 113(34), pp. E5062–E5071. Available at: https://doi.org/10.1073/PNAS.1609157113/SUPPL_FILE/PNAS.201609157SI.PDF.
Viennet, E. et al. (2025) ‘Blood under pressure: how climate change threatens blood safety and supply chains’, The Lancet Planetary Health, 9(4), pp. e304–e313. Available at: https://doi.org/10.1016/S2542-5196(25)00051-8.
Vieno, M. et al. (2016) ‘The UK particulate matter air pollution episode of March–April 2014: more than Saharan dust’, Environmental Research Letters, 11(4), pp. 044004–044004. Available at: https://doi.org/10.1088/1748-9326/11/4/044004.
Walker, A.R. (2003) Ticks of domestic animals in Africa: a guide to identification of species. Bioscience Reports Edinburgh. Available at: https://www.researchgate.net/profile/Ali-Bouattour/publication/294560744_Tiques_d’importance_medicale_et_veterinaire_le_bassin_mediterraneen_ICTTD_CD-ROM_Mediterraneans_ticks_3-12_12/links/5fca11ab45851568d13a9198/Tiques-dimportance-medicale-et-veterinaire-le-bassin-mediterraneen-ICTTD-CD-ROM-Mediterraneans-ticks-3-12-12.pdf (Accessed: 8 February 2026).
Wan, K. et al. (2022) ‘Temperature-related mortality and associated vulnerabilities: evidence from Scotland using extended time-series datasets’, Environmental Health: A Global Access Science Source, 21(1), pp. 1–14. Available at: https://doi.org/10.1186/S12940-022-00912-5/FIGURES/5.
Wang, R. et al. (2023) ‘Exploring mechanistic pathways linking urban green and blue space to mental wellbeing before and after urban regeneration of a greenway: Evidence from the Connswater Community Greenway, Belfast, UK’, Landscape and Urban Planning, 235, pp. 104739–104739. Available at: https://doi.org/10.1016/J.LANDURBPLAN.2023.104739.
Wang, R. et al. (2024) ‘How Do Awareness, Perceptions, and Expectations of an Urban Greenway Influence Residents’ Visits and Recreational Physical Activity? Evidence From the Connswater Community Greenway, Belfast, Northern Ireland’, Leisure Sciences [Preprint]. Available at: https://doi.org/10.1080/01490400.2024.2335918.
Welsh Government (2015a) Water strategy for Wales. Welsh Government. Available at: https://www.gov.wales/water-strategy (Accessed: 8 February 2026).
Welsh Government (2015b) Well-being of Future Generations (Wales) Act 2015. Text. Statute Law Database. Available at: https://www.legislation.gov.uk/anaw/2015/2/contents (Accessed: 8 February 2026).
Welsh Government (2019) ‘Prosperity for all: a climate conscious Wales’, www.gov.wales [Preprint]. Available at: https://www.gov.wales/prosperity-all-climate-conscious-wales.
Welsh Government (2020) ‘National Strategy for Flood and Coastal Erosion Risk Management in Wales’, www.gov.wales [Preprint]. Available at: https://www.gov.wales/national-strategy-flood-and-coastal-erosion-risk-management-wales.
Welsh Government (2023a) Healthy weight strategy (Healthy Weight Healthy Wales). Available at: https://www.gov.wales/healthy-weight-strategy-healthy-weight-healthy-wales (Accessed: 8 February 2026).
Welsh Government (2023b) ‘Welsh Housing Quality Standard 2023’, www.gov.wales [Preprint]. Available at: https://www.gov.wales/welsh-housing-quality-standard-2023-0.
Welsh Government (2024a) Child Poverty Strategy for Wales 2024. Welsh Government. Available at: https://www.gov.wales/child-poverty-strategy-wales-2024 (Accessed: 8 February 2026).
Welsh Government (2024b) Climate Adaptation Strategy for Wales 2024. Welsh Government. Available at: https://www.gov.wales/climate-adaptation-strategy-wales-2024.
Welsh Government (2024c) Environment (Air Quality and Soundscapes) (Wales) Act 2024. Available at: https://www.legislation.gov.uk/asc/2024/2 (Accessed: 6 February 2026).
Welsh Government (2024d) ‘Health and Social Care Climate Adaptation Toolkit – Guidance for building climate resilient health and social care in Wales’, www.gov.wales [Preprint]. Available at: https://www.gov.wales/health-and-social-care-climate-adaptation-toolkit.
Welsh Government (2024e) ‘Planning Policy Wales’, www.gov.wales [Preprint]. Available at: https://www.gov.wales/planning-policy-wales.
Welsh Government (2025a) Building regulations guidance: part F (ventilation). Welsh Government. Available at: https://www.gov.wales/approved-document-f-ventilation.
Welsh Government (2025b) Community Food Strategy. Welsh Government. Available at: https://www.gov.wales/community-food-strategy (Accessed: 8 February 2026).
Welsh Government (2025c) ‘Health and social care climate emergency national programme’, www.gov.wales [Preprint]. Available at: https://www.gov.wales/health-and-social-care-climate-emergency-national-programme.
White, M.P. et al. (2020) ‘Blue space, health and well-being: A narrative overview and synthesis of potential benefits’, Environmental Research, 191, pp. 110169–110169. Available at: https://doi.org/10.1016/J.ENVRES.2020.110169.
Williamson, Nunn, J. and Pearce, H. (2021) Air Pollution and Inequalities in London: 2019. Greater London Authority. Available at: https://www.london.gov.uk/programmes-and-strategies/environment-and-climate-change/environment-publications/air-pollution-and-inequalities-london-2019.
Withers, A.J. et al. (2024) ‘Using correlative and mechanistic species distribution models to predict vector-borne disease risk for the current and future environmental and climatic change: a case study of West Nile Virus in the UK’, bioRxiv, p. 2024.09.12.612656-2024.09.12.612656. Available at: https://doi.org/10.1101/2024.09.12.612656.
Woodland Trust, American Forests, and Centre for Sustainable Healthcare (2023) ‘Tree Equity Score UK Map’, https://uk.treeequityscore.org [Preprint]. Available at: https://uk.treeequityscore.org/map.
Young, S. and Bergseng, A.M. (2020) ‘Delivering social care in a changing climate’, www.climateexchange.org.uk [Preprint]. Available at: www.climatexchange.org.uk.
Zhang, S. et al. (2024) ‘Effect modification of air pollution on the association between heat and mortality in five European countries’, Environmental Research, 263, pp. 120023–120023. Available at: https://doi.org/10.1016/j.envres.2024.120023.
Zhao, J. et al. (2024) ‘Long-term prediction of the effects of climate change on indoor climate and air quality’, Environmental Research, 243, pp. 117804–117804. Available at: https://doi.org/10.1016/J.ENVRES.2023.117804.
Zhao, J. et al. (2025) ‘Long-term prediction of climate change impacts on indoor particle pollution-case study of a residential building in Germany †’. Available at: https://doi.org/10.1039/d4em00663a.
Downloads
-

CCRA4 Technical Report – Chapter 3 – Health and Wellbeing
Type: PDF (2 MB)
Share on: